

Multimodal assessment improves neuroprognosis performance in clinically unresponsive critical-care patients with brain injury
- PMID: 38816609
- PMCID: PMC11333287
- DOI: 10.1038/s41591-024-03019-1
Multimodal assessment improves neuroprognosis performance in clinically unresponsive critical-care patients with brain injury
Abstract
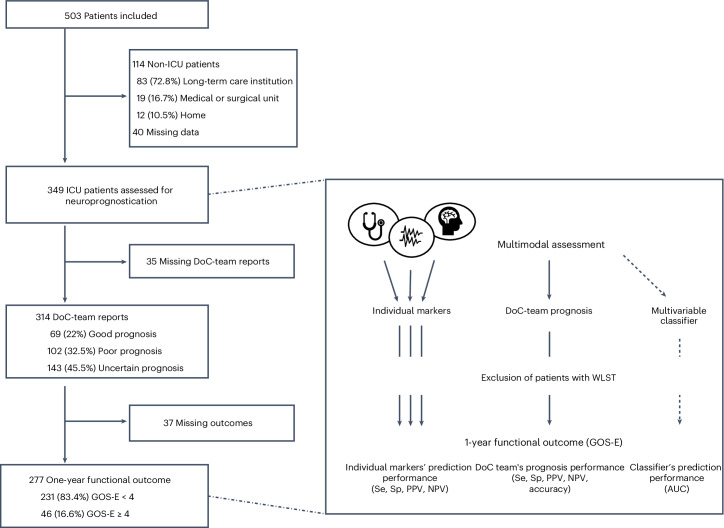
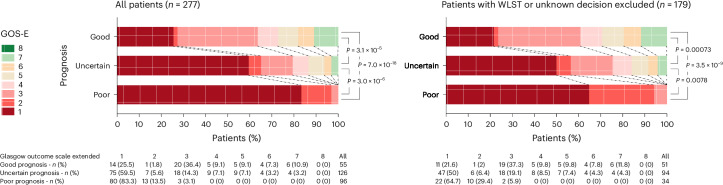
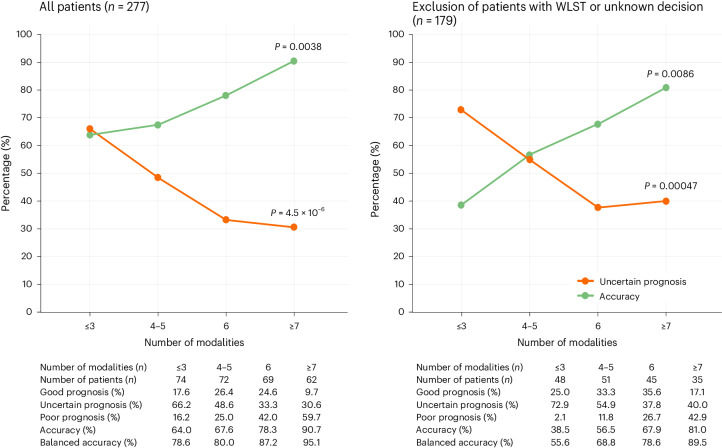
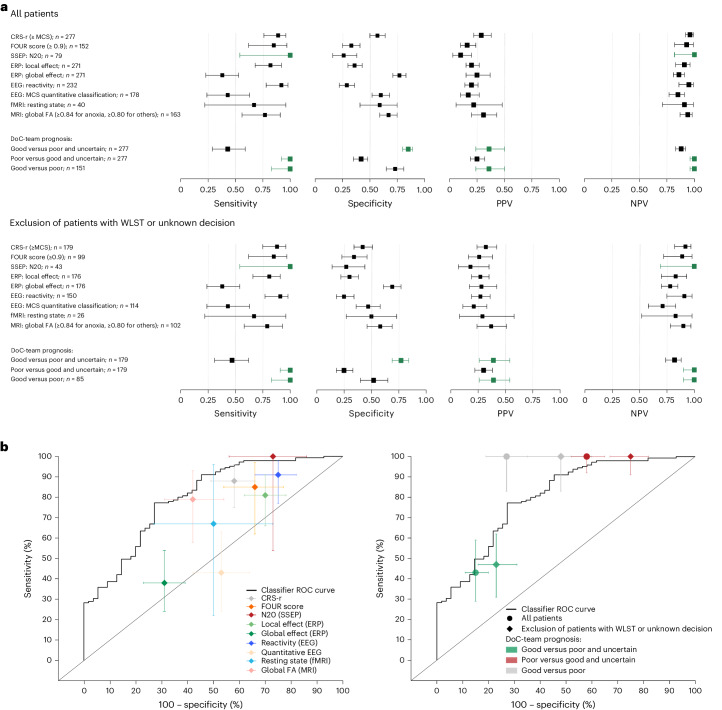
Accurately predicting functional outcomes for unresponsive patients with acute brain injury is a medical, scientific and ethical challenge. This prospective study assesses how a multimodal approach combining various numbers of behavioral, neuroimaging and electrophysiological markers affects the performance of outcome predictions. We analyzed data from 349 patients admitted to a tertiary neurointensive care unit between 2009 and 2021, categorizing prognoses as good, uncertain or poor, and compared these predictions with observed outcomes using the Glasgow Outcome Scale-Extended (GOS-E, levels ranging from 1 to 8, with higher levels indicating better outcomes). After excluding cases with life-sustaining therapy withdrawal to mitigate the self-fulfilling prophecy bias, our findings reveal that a good prognosis, compared with a poor or uncertain one, is associated with better one-year functional outcomes (common odds ratio (95% CI) for higher GOS-E: OR = 14.57 (5.70-40.32), P < 0.001; and 2.9 (1.56-5.45), P < 0.001, respectively). Moreover, increasing the number of assessment modalities decreased uncertainty (OR = 0.35 (0.21-0.59), P < 0.001) and improved prognostic accuracy (OR = 2.72 (1.18-6.47), P = 0.011). Our results underscore the value of multimodal assessment in refining neuroprognostic precision, thereby offering a robust foundation for clinical decision-making processes for acutely brain-injured patients. ClinicalTrials.gov registration: NCT04534777 .
© 2024. The Author(s).
Conflict of interest statement
J.D.S. and L.N. are shareholders and co-founders of Neurometers; L.P. is a shareholder and co-founder of Braintale. The other authors declare no competing interests.
Figures



Comment in
-
What criteria for neuropronostication: consciousness or ability? The neuro-intensivist's dilemma.Crit Care. 2024 Oct 3;28(1):322. doi: 10.1186/s13054-024-05098-5. Crit Care. 2024. PMID: 39363377 Free PMC article. No abstract available.
References
-
- Giacino, J. T. & Edlow, B. L. Covert consciousness in the intensive care unit. Trends Neurosci.42, 844–847 (2019). - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
