

Mortality, morbidity & clinical outcome with different types of vasopressors in out of hospital cardiac arrest patients- a systematic review and meta-analysis
- PMID: 38816786
- PMCID: PMC11137957
- DOI: 10.1186/s12872-024-03962-4
Mortality, morbidity & clinical outcome with different types of vasopressors in out of hospital cardiac arrest patients- a systematic review and meta-analysis
Abstract
Background & objective: Despite their continued use, the effectiveness and safety of vasopressors in post-cardiac arrest patients remain controversial. This study examined the efficacy of various vasopressors in cardiac arrest patients in terms of clinical, morbidity, and mortality outcomes.
Methods: A comprehensive literature search was performed using online databases (MeSH terms: MEDLINE (Ovid), CENTRAL (Cochrane Library), Embase (Ovid), CINAHL, Scopus, and Google Scholar) from 1997 to 2023 for relevant English language studies. The primary outcomes of interest for this study included short-term survival leading to death, return of spontaneous circulation (ROSC), survival to hospital discharge, neurological outcomes, survival to hospital admission, myocardial infarction, and incidence of arrhythmias.
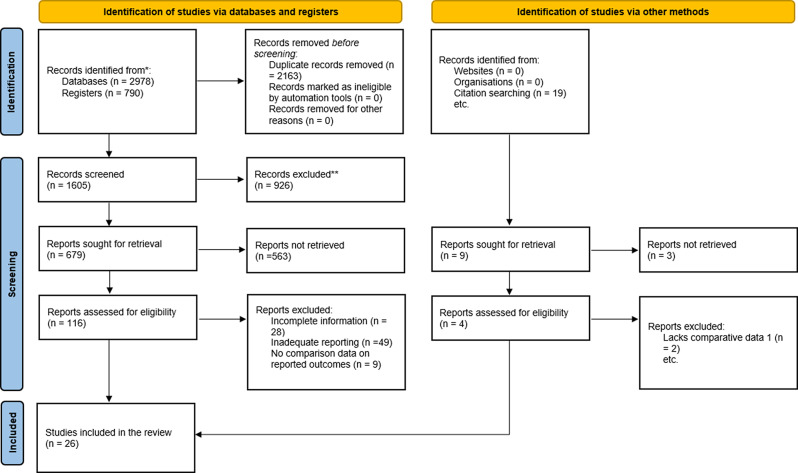
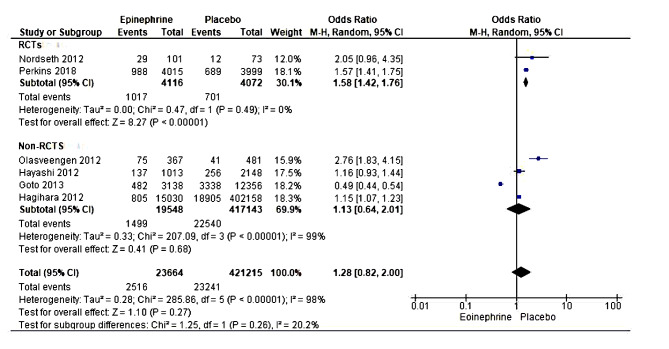
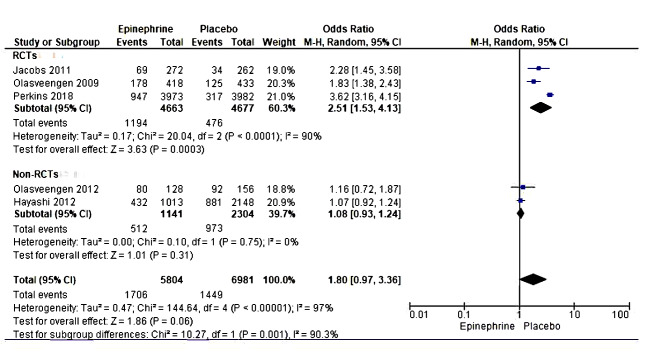
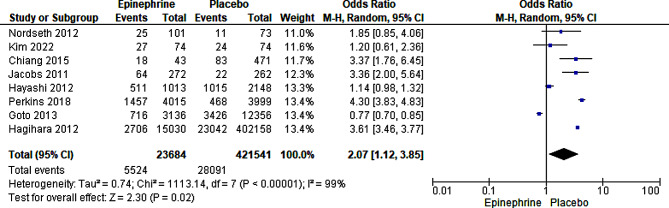
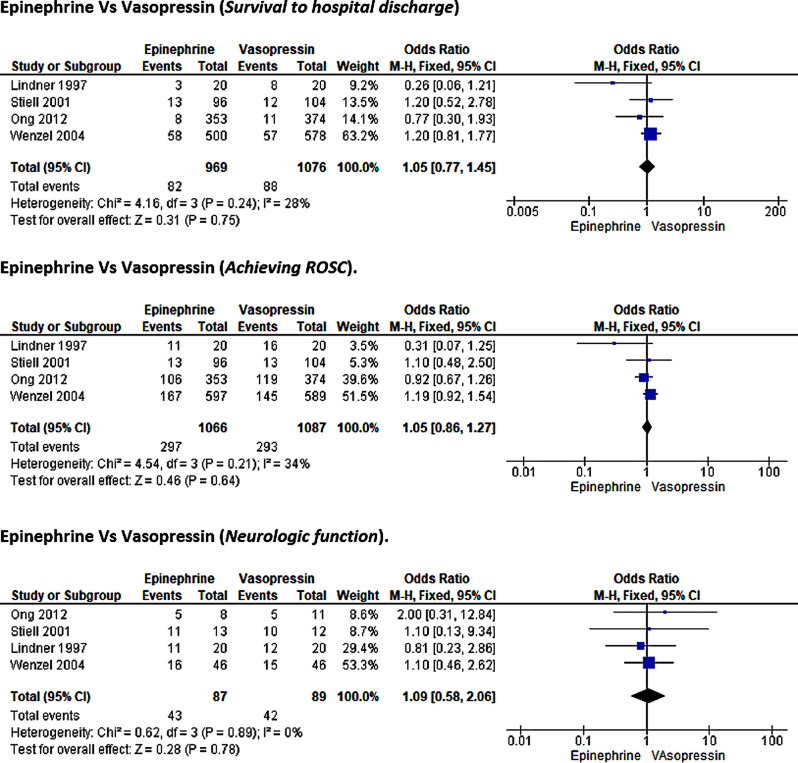
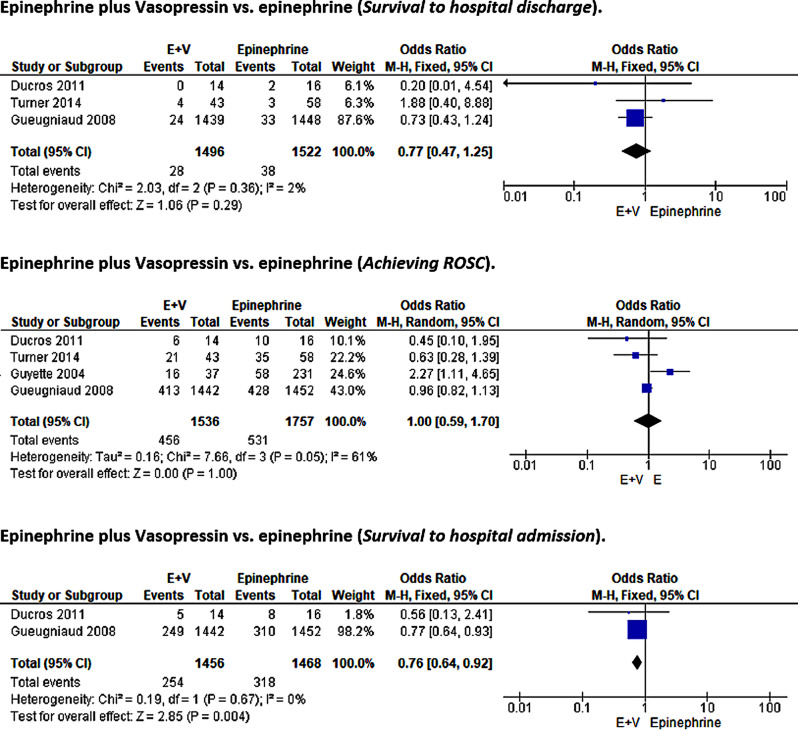
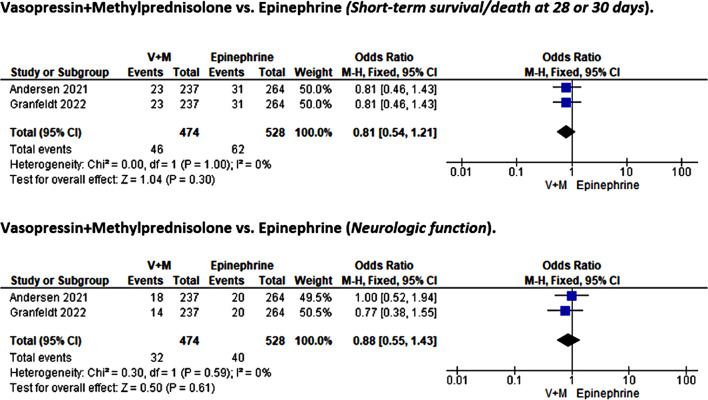
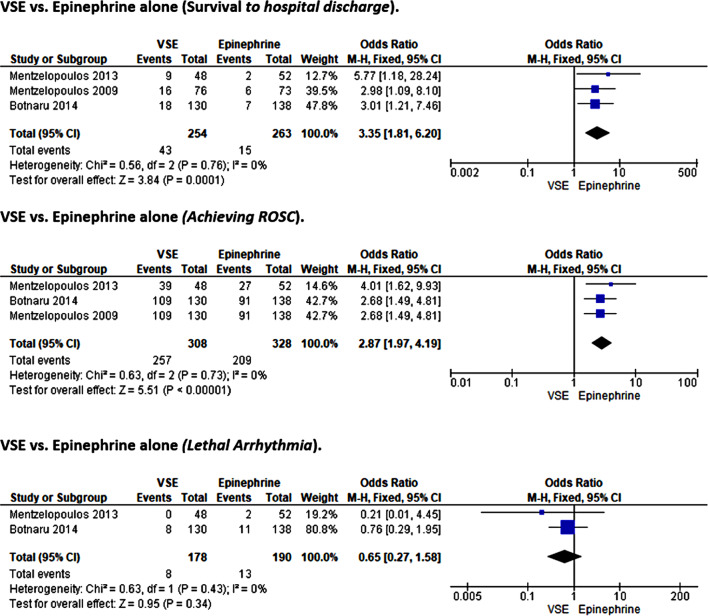
Results: In this meta-analysis, 26 studies, including 16 RCTs and ten non-RCTs, were evaluated. The focus was on the efficacy of epinephrine, vasopressin, methylprednisolone, dopamine, and their combinations in medical emergencies. Epinephrine treatment was associated with better odds of survival to hospital discharge (OR = 1.52, 95%CI [1.20, 1.94]; p < 0.001) and achieving ROSC (OR = 3.60, 95% CI [3.45, 3.76], P < 0.00001)) over placebo but not in other outcomes of interest such as short-term survival/ death at 28-30 days, survival to hospital admission, or neurological function. In addition, our analysis indicates non-superiority of vasopressin or epinephrine vasopressin-plus-epinephrine therapy over epinephrine monotherapy except for survival to hospital admission where the combinatorial therapy was associated with better outcome (0.76, 95%CI [0.64, 0.92]; p = 0.004). Similarly, we noted the non-superiority of vasopressin-plus-methylprednisolone versus placebo. Finally, while higher odds of survival to hospital discharge (OR = 3.35, 95%CI [1.81, 6.2]; p < 0.001) and ROSC (OR = 2.87, 95%CI [1.97, 4.19]; p < 0.001) favoring placebo over VSE therapy were observed, the risk of lethal arrhythmia was not statistically significant. There was insufficient literature to assess the effects of dopamine versus other treatment modalities meta-analytically.
Conclusion: This meta-analysis indicated that only epinephrine yielded superior outcomes among vasopressors than placebo, albeit limited to survival to hospital discharge and ROSC. Additionally, we demonstrate the non-superiority of vasopressin over epinephrine, although vasopressin could not be compared to placebo due to the paucity of data. The addition of vasopressin to epinephrine treatment only improved survival to hospital admission.
Keywords: Cardiac arrest; Cardiopulmonary resuscitation; Ionotropic; ROSC; Return of spontaneous circulation; Vasopressors.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
Comparison between norepinephrine plus epinephrine and norepinephrine plus vasopressin after return of spontaneous circulation in patients with out-of-hospital cardiac arrest.Sci Rep. 2025 Apr 18;15(1):13375. doi: 10.1038/s41598-025-96857-z. Sci Rep. 2025. PMID: 40251260 Free PMC article.
-
Adrenaline and vasopressin for cardiac arrest.Cochrane Database Syst Rev. 2019 Jan 17;1(1):CD003179. doi: 10.1002/14651858.CD003179.pub2. Cochrane Database Syst Rev. 2019. PMID: 30653257 Free PMC article.
-
Vasopressin, steroids, and epinephrine and neurologically favorable survival after in-hospital cardiac arrest: a randomized clinical trial.JAMA. 2013 Jul 17;310(3):270-9. doi: 10.1001/jama.2013.7832. JAMA. 2013. PMID: 23860985 Clinical Trial.
-
Comparison of different treatments of out-of-hospital cardiac arrest: A systematic review and network meta-analysis.Medicine (Baltimore). 2025 Mar 7;104(10):e41698. doi: 10.1097/MD.0000000000041698. Medicine (Baltimore). 2025. PMID: 40068023 Free PMC article.
-
Therapeutic effects of vasopressin on cardiac arrest: a systematic review and meta-analysis.BMJ Open. 2023 Apr 17;13(4):e065061. doi: 10.1136/bmjopen-2022-065061. BMJ Open. 2023. PMID: 37068900 Free PMC article.
Cited by
-
Use of Epinephrine in Cardiac Arrest: Advances and Future Challenges.Medicina (Kaunas). 2024 Nov 20;60(11):1904. doi: 10.3390/medicina60111904. Medicina (Kaunas). 2024. PMID: 39597089 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
