

Effectiveness of nirmatrelvir/ritonavir and molnupiravir in non-hospitalized adults with COVID-19: systematic review and meta-analysis of observational studies
- PMID: 38817046
- PMCID: PMC11368430
- DOI: 10.1093/jac/dkae163
Effectiveness of nirmatrelvir/ritonavir and molnupiravir in non-hospitalized adults with COVID-19: systematic review and meta-analysis of observational studies
Abstract
Objective: To determine the effectiveness of nirmatrelvir/ritonavir and molnupiravir among vaccinated and unvaccinated non-hospitalized adults with COVID-19.
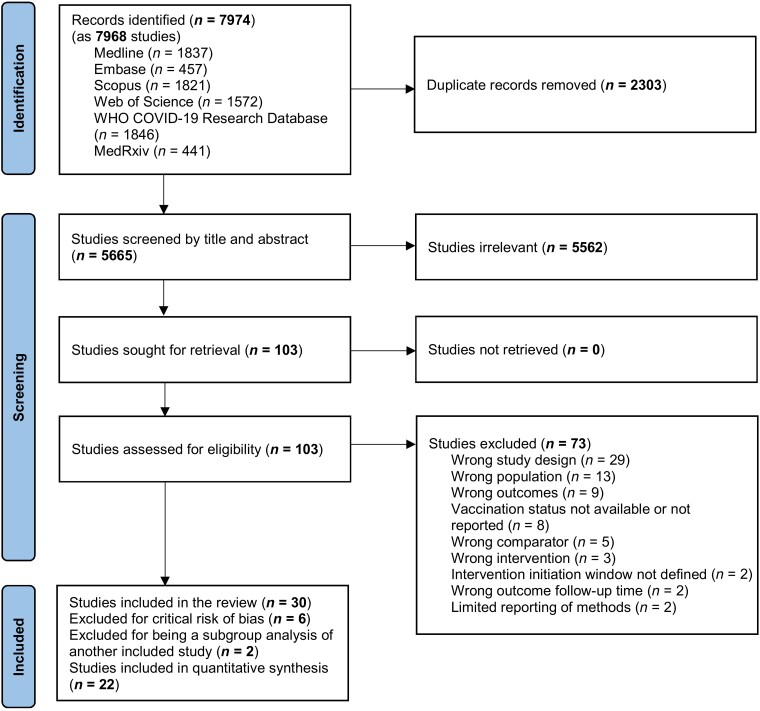
Methods: Observational studies of nirmatrelvir/ritonavir or molnupiravir compared to no antiviral drug treatment for COVID-19 in non-hospitalized adults with data on vaccination status were included. We searched MEDLINE, EMBASE, Scopus, Web of Science, WHO COVID-19 Research Database and medRxiv for reports published between 1 January 2022 and 8 November 2023. The primary outcome was a composite of hospitalization or mortality up to 35 days after COVID-19 diagnosis. Risk of bias was assessed with ROBINS-I. Risk ratios (RR), hazard ratios (HR) and risk differences (RD) were separately estimated using random-effects models.
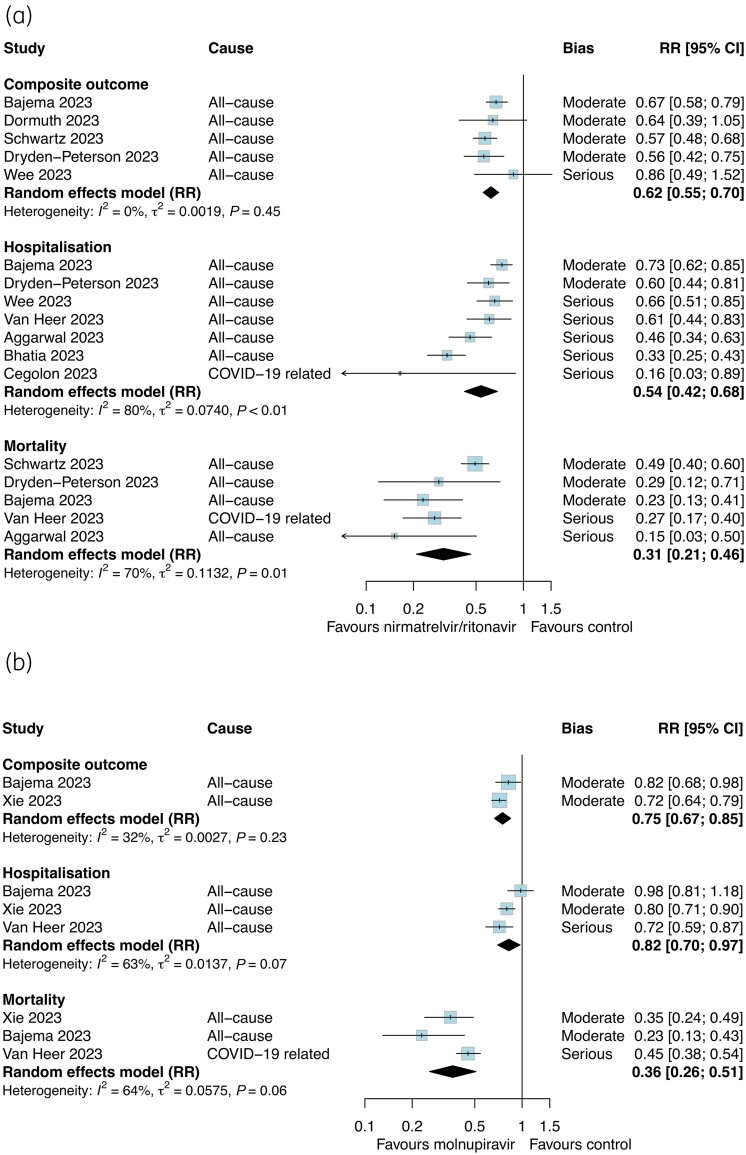
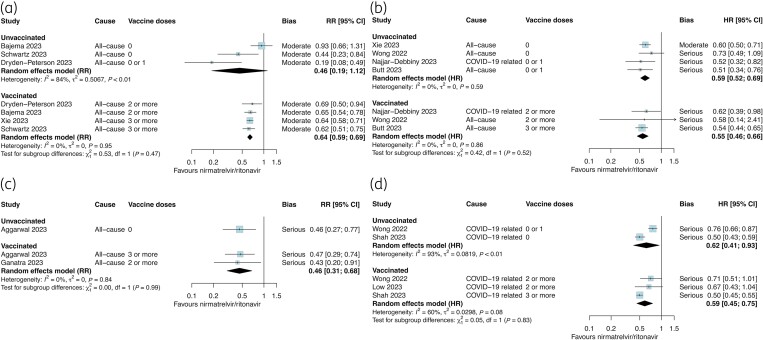
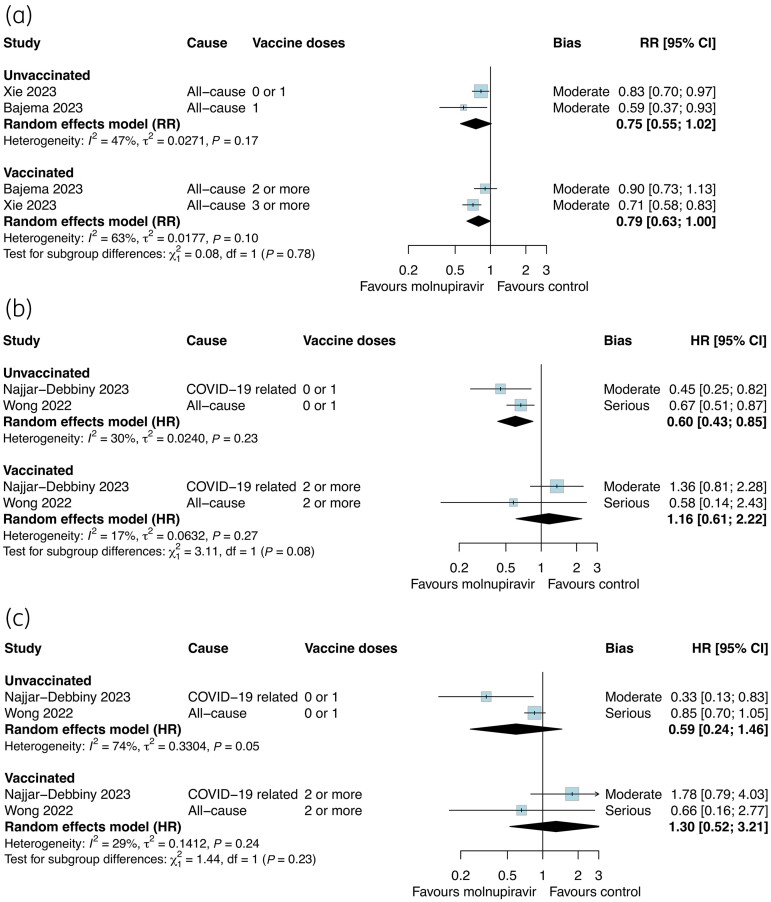
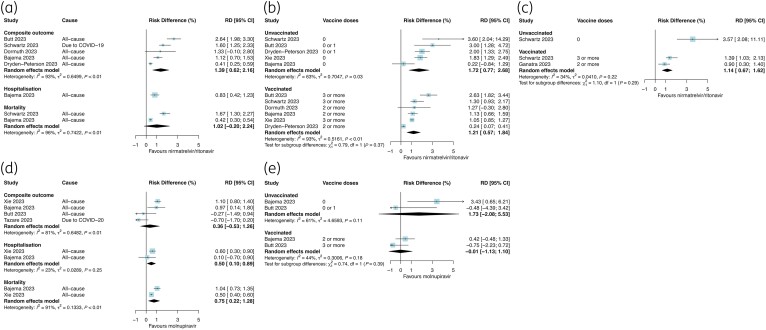
Results: We included 30 cohort studies on adults treated with nirmatrelvir/ritonavir (n = 462 279) and molnupiravir (n = 48 008). Nirmatrelvir/ritonavir probably reduced the composite outcome (RR 0.62, 95%CI 0.55-0.70; I2 = 0%; moderate certainty) with no evidence of effect modification by vaccination status (RR Psubgroup = 0.47). In five studies, RD estimates against the composite outcome for nirmatrelvir/ritonavir were 1.21% (95%CI 0.57% to 1.84%) in vaccinated and 1.72% (95%CI 0.59% to 2.85%) in unvaccinated subgroups.Molnupiravir may slightly reduce the composite outcome (RR 0.75, 95%CI 0.67-0.85; I2 = 32%; low certainty). Evidence of effect modification by vaccination status was inconsistent among studies reporting different effect measures (RR Psubgroup = 0.78; HR Psubgroup = 0.08). In two studies, RD against the composite outcome for molnupiravir were -0.01% (95%CI -1.13% to 1.10%) in vaccinated and 1.73% (95%CI -2.08% to 5.53%) in unvaccinated subgroups.
Conclusions: Among cohort studies of non-hospitalized adults with COVID-19, nirmatrelvir/ritonavir is effective against the composite outcome of severe COVID-19 independent of vaccination status. Further research and a reassessment of molnupiravir use among vaccinated adults are warranted.
Registration: PROSPERO CRD42023429232.
© The Author(s) 2024. Published by Oxford University Press on behalf of British Society for Antimicrobial Chemotherapy.
Figures
Similar articles
-
Real-world effectiveness of nirmatrelvir-ritonavir and molnupiravir in non-hospitalized adults with COVID-19: a population-based, retrospective cohort study.Clin Microbiol Infect. 2025 Mar;31(3):451-458. doi: 10.1016/j.cmi.2024.10.026. Epub 2024 Nov 4. Clin Microbiol Infect. 2025. PMID: 39505067
-
Comparing the effectiveness of molnupiravir and nirmatrelvir-ritonavir in non-hospitalized and hospitalized COVID-19 patients with type 2 diabetes: A target trial emulation study.Diabetes Obes Metab. 2024 Oct;26(10):4653-4664. doi: 10.1111/dom.15830. Epub 2024 Aug 7. Diabetes Obes Metab. 2024. PMID: 39109461
-
Effectiveness of nirmatrelvir/ritonavir and molnupiravir on post-COVID-19 outcomes among outpatients: a target trial emulation investigation.Emerg Microbes Infect. 2025 Dec;14(1):2469648. doi: 10.1080/22221751.2025.2469648. Epub 2025 Mar 4. Emerg Microbes Infect. 2025. PMID: 39964106 Free PMC article.
-
Early use of oral antiviral drugs and the risk of post COVID-19 syndrome: A systematic review and network meta-analysis.J Infect. 2024 Aug;89(2):106190. doi: 10.1016/j.jinf.2024.106190. Epub 2024 Jun 2. J Infect. 2024. PMID: 38834107
-
Nirmatrelvir/Ritonavir Regimen for Mild/Moderately Severe COVID-19: A Rapid Review With Meta-Analysis and Trial Sequential Analysis.Ann Fam Med. 2024 Jul-Aug;22(4):336-346. doi: 10.1370/afm.3120. Ann Fam Med. 2024. PMID: 39038972 Free PMC article.
Cited by
-
Joint analysis of time-varying effect of vaccine and antiviral drug for preventing severe complications and mortality.Sci Rep. 2025 Feb 15;15(1):5640. doi: 10.1038/s41598-025-89043-8. Sci Rep. 2025. PMID: 39955370 Free PMC article.
-
Cost-Effectiveness Analysis of Molnupiravir Versus Best Supportive Care for the Treatment of Outpatient COVID-19 in High-Risk Older Adults in Japan.Pharmacoecon Open. 2025 Jul;9(4):571-584. doi: 10.1007/s41669-025-00578-y. Epub 2025 Apr 23. Pharmacoecon Open. 2025. PMID: 40266489 Free PMC article.
References
-
- Mathieu E, Ritchie H, Rodés-Guirao Let al. . Coronavirus Pandemic (COVID-19) [online]. 2020. https://ourworldindata.org/coronavirus
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
