

Evaluating effectiveness and safety of combined percutaneous transhepatic gallbladder drainage and laparoscopic cholecystectomy in acute cholecystitis patients: Meta-analysis
- PMID: 38817274
- PMCID: PMC11135318
- DOI: 10.4240/wjgs.v16.i5.1407
Evaluating effectiveness and safety of combined percutaneous transhepatic gallbladder drainage and laparoscopic cholecystectomy in acute cholecystitis patients: Meta-analysis
Abstract
Background: Acute cholecystitis (AC) is a common disease in general surgery. Laparoscopic cholecystectomy (LC) is widely recognized as the "gold standard" surgical procedure for treating AC. For low-risk patients without complications, LC is the recommended treatment plan, but there is still controversy regarding the treatment strategy for moderate AC patients, which relies more on the surgeon's experience and the medical platform of the visiting unit. Percutaneous transhepatic gallbladder puncture drainage (PTGBD) can effectively alleviate gallbladder inflammation, reduce gallbladder wall edema and adhesion around the gallbladder, and create a "time window" for elective surgery.
Aim: To compare the clinical efficacy and safety of LC or PTGBD combined with LC for treating AC patients, providing a theoretical basis for choosing reasonable surgical methods for AC patients.
Methods: In this study, we conducted a clinical investigation regarding the combined use of PTGBD tubes for the treatment of gastric cancer patients with AC. We performed searches in the following databases: PubMed, Web of Science, EMBASE, Cochrane Library, China National Knowledge Infrastructure, and Wanfang Database. The search encompassed literature published from the inception of these databases to the present. Subsequently, relevant data were extracted, and a meta-analysis was conducted using RevMan 5.3 software.
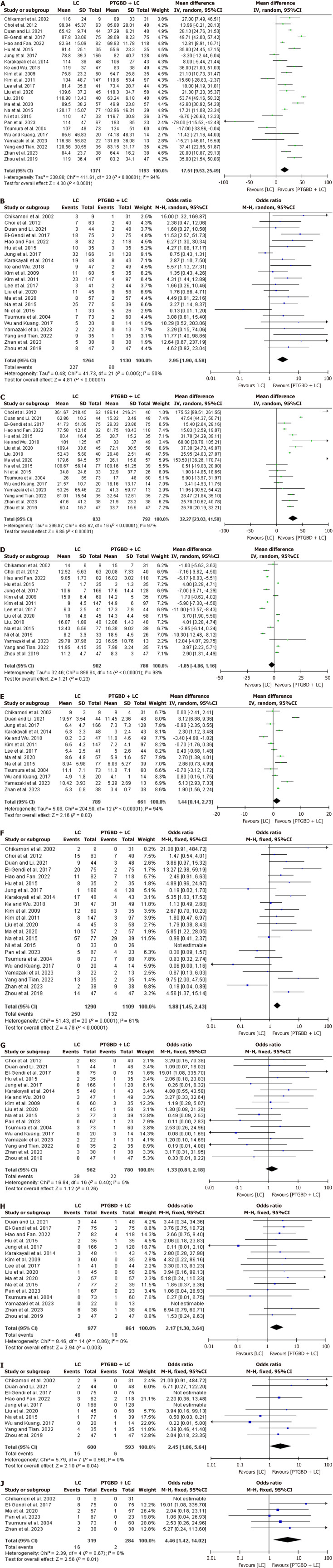
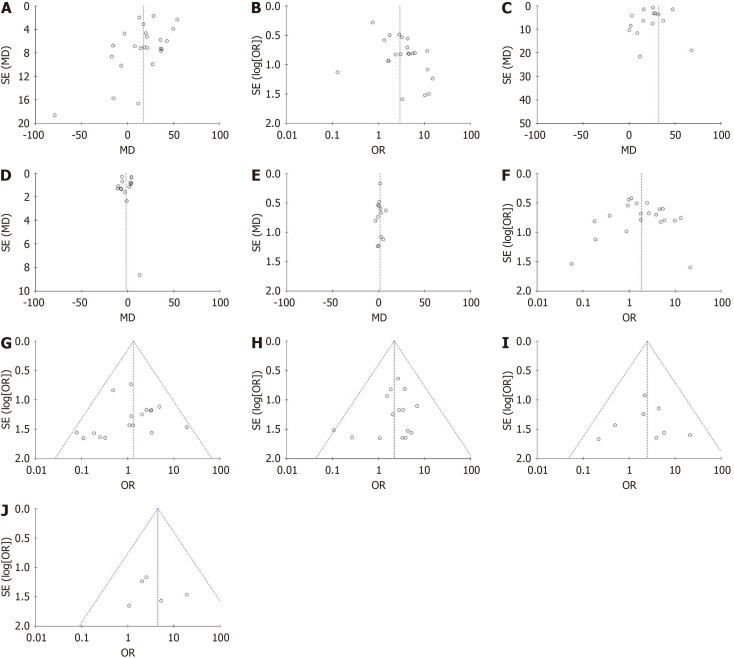
Results: A comprehensive analysis was conducted, encompassing 24 studies involving a total of 2564 patients. These patients were categorized into two groups: 1371 in the LC group and 1193 in the PTGBD + LC group. The outcomes of the meta-analysis revealed noteworthy disparities between the PTGBD + LC group and the LC group in multiple dimensions: (1) Operative time: Mean difference (MD) = 17.51, 95%CI: 9.53-25.49, P < 0.01; (2) Conversion to open surgery rate: Odds ratio (OR) = 2.95, 95%CI: 1.90-4.58, P < 0.01; (3) Intraoperative bleeding loss: MD = 32.27, 95%CI: 23.03-41.50, P < 0.01; (4) Postoperative hospital stay: MD = 1.44, 95%CI: 0.14-2.73, P = 0.03; (5) Overall postoperative complication rate: OR = 1.88, 95%CI: 1.45-2.43, P < 0.01; (6) Bile duct injury: OR = 2.17, 95%CI: 1.30-3.64, P = 0.003; (7) Intra-abdominal hemorrhage: OR = 2.45, 95%CI: 1.06-5.64, P = 0.004; and (8) Wound infection: OR = 0. These findings consistently favored the PTGBD + LC group over the LC group. There were no significant differences in the total duration of hospitalization [MD = -1.85, 95%CI: -4.86-1.16, P = 0.23] or bile leakage [OR = 1.33, 95%CI: 0.81-2.18, P = 0.26] between the two groups.
Conclusion: The combination of PTGBD tubes with LC for AC treatment demonstrated superior clinical efficacy and enhanced safety, suggesting its broader application value in clinical practice.
Keywords: Acute cholecystitis; Efficacy; Laparoscopic cholecystectomy; Meta-analysis; Percutaneous transhepatic gallbladder drainage.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures
Similar articles
-
Percutaneous Transhepatic Gallbladder Drainage Combined with Laparoscopic Cholecystectomy Versus Emergency Laparoscopic Cholecystectomy for the Treatment of Moderate Acute Cholecystitis: A Meta-Analysis.J Laparoendosc Adv Surg Tech A. 2022 Jul;32(7):733-739. doi: 10.1089/lap.2021.0579. Epub 2021 Nov 9. J Laparoendosc Adv Surg Tech A. 2022. PMID: 34748409
-
Urgent Versus Elective Laparoscopic Cholecystectomy Following Percutaneous Transhepatic Gallbladder Drainage for Moderate Acute Cholecystitis: A Meta-Analysis.Surg Innov. 2025 Feb;32(1):25-35. doi: 10.1177/15533506241300735. Epub 2024 Nov 18. Surg Innov. 2025. PMID: 39556004
-
Delayed Laparoscopic Cholecystectomy After Percutaneous Transhepatic Gallbladder Drainage Versus Emergency Laparoscopic Cholecystectomy for Acute Cholecystitis: A Meta-Analysis.Turk J Gastroenterol. 2021 Nov;32(11):945-955. doi: 10.5152/tjg.2021.20578. Turk J Gastroenterol. 2021. PMID: 34872896 Free PMC article.
-
Management of Acute Cholecystitis in High-Risk Patients: Percutaneous Gallbladder Drainage as a Definitive Treatment vs. Emergency Cholecystectomy-Systematic Review and Meta-Analysis.J Clin Med. 2023 Jul 26;12(15):4903. doi: 10.3390/jcm12154903. J Clin Med. 2023. PMID: 37568306 Free PMC article. Review.
-
Comparison of the safety and effectiveness of different surgical timing for acute cholecystitis after percutaneous transhepatic gallbladder drainage: a systematic review and meta-analysis.Langenbecks Arch Surg. 2023 Mar 21;408(1):125. doi: 10.1007/s00423-023-02861-0. Langenbecks Arch Surg. 2023. PMID: 36943587
References
-
- Choi JH, Kim HW, Lee JC, Paik KH, Seong NJ, Yoon CJ, Hwang JH, Kim J. Percutaneous transhepatic versus EUS-guided gallbladder drainage for malignant cystic duct obstruction. Gastrointest Endosc. 2017;85:357–364. - PubMed
-
- Pisano M, Allievi N, Gurusamy K, Borzellino G, Cimbanassi S, Boerna D, Coccolini F, Tufo A, Di Martino M, Leung J, Sartelli M, Ceresoli M, Maier RV, Poiasina E, De Angelis N, Magnone S, Fugazzola P, Paolillo C, Coimbra R, Di Saverio S, De Simone B, Weber DG, Sakakushev BE, Lucianetti A, Kirkpatrick AW, Fraga GP, Wani I, Biffl WL, Chiara O, Abu-Zidan F, Moore EE, Leppäniemi A, Kluger Y, Catena F, Ansaloni L. 2020 World Society of Emergency Surgery updated guidelines for the diagnosis and treatment of acute calculus cholecystitis. World J Emerg Surg. 2020;15:61. - PMC - PubMed
-
- Yamada K, Yamashita Y, Yamada T, Takeno S, Noritomi T. Optimal timing for performing percutaneous transhepatic gallbladder drainage and subsequent cholecystectomy for better management of acute cholecystitis. J Hepatobiliary Pancreat Sci. 2015;22:855–861. - PubMed
-
- Sanaiha Y, Juo YY, Rudasill SE, Jaman R, Sareh S, de Virgilio C, Benharash P. Percutaneous cholecystostomy for grade III acute cholecystitis is associated with worse outcomes. Am J Surg. 2020;220:197–202. - PubMed
LinkOut - more resources
Full Text Sources
