

Scapholunate Ligament Injuries
- PMID: 38817761
- PMCID: PMC11133945
- DOI: 10.1016/j.jhsg.2024.01.015
Scapholunate Ligament Injuries
Abstract
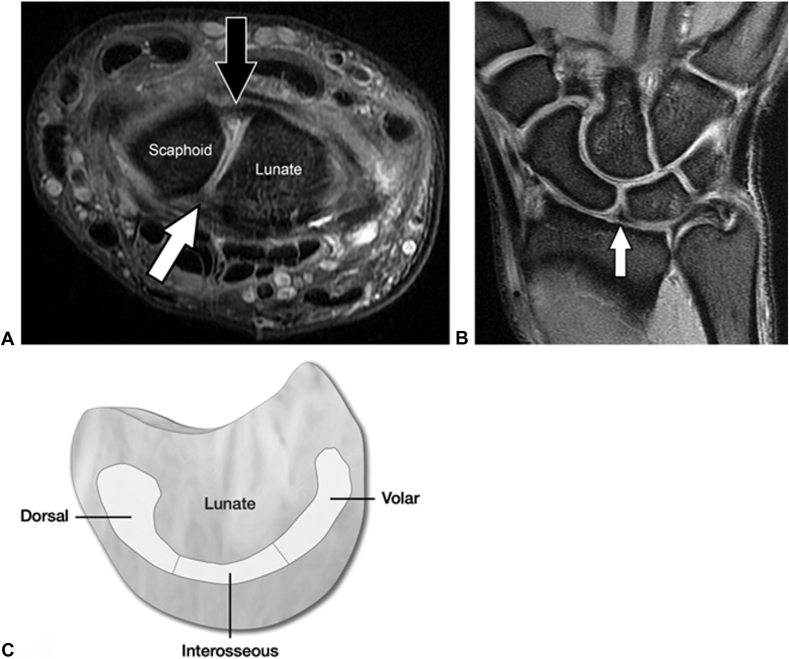
Injuries to the scapholunate interosseous ligament (SLIL) complex can result in a predictable cascade of incongruous motion in the carpus that leads to radiocarpal degeneration. Both acute traumatic impact and repetitive motion can render the SLIL insufficient. A thorough understanding of SLIL anatomy is required for appropriate diagnosis and treatment. Here, we review scapholunate ligament anatomy, prevention strategies, methods of diagnosis, nonoperative and operative treatments, and outcomes. A myriad of treatment options exist for each stage of the SLIL injury, and management should be an open discussion between the patient and physician.
Keywords: Anatomy; Diagnosis; Prevention; Scapholunate interosseous ligament complex injuries; Treatment.
© 2024 The Authors.
Conflict of interest statement
No benefits in any form have been received or will be received related directly to this article.
Figures






Similar articles
-
The Quantitative Anatomy of the Dorsal Scapholunate Interosseous Ligament.Hand (N Y). 2019 Jan;14(1):80-85. doi: 10.1177/1558944718798846. Epub 2018 Sep 12. Hand (N Y). 2019. PMID: 30205714 Free PMC article.
-
Cadaveric Testing of a Novel Scapholunate Ligament Reconstruction.J Wrist Surg. 2018 Apr;7(2):141-147. doi: 10.1055/s-0037-1607326. Epub 2017 Oct 26. J Wrist Surg. 2018. PMID: 29576920 Free PMC article.
-
The Anatomy of the Dorsal Capsulo-Scapholunate Septum: A Cadaveric Study.J Wrist Surg. 2017 Aug;6(3):244-247. doi: 10.1055/s-0036-1597922. Epub 2017 Jan 5. J Wrist Surg. 2017. PMID: 28725508 Free PMC article.
-
Scapholunate Interosseous Ligament Anatomy and Biomechanics.J Hand Surg Am. 2015 Aug;40(8):1692-702. doi: 10.1016/j.jhsa.2015.03.032. Epub 2015 Jul 1. J Hand Surg Am. 2015. PMID: 26143029 Review.
-
Scapholunate Instability: Diagnosis and Management - Anatomy, Kinematics, and Clinical Assessment - Part I.J Hand Surg Am. 2023 Nov;48(11):1139-1149. doi: 10.1016/j.jhsa.2023.05.013. Epub 2023 Jul 14. J Hand Surg Am. 2023. PMID: 37452815 Review.
Cited by
-
Physiotherapy Rehabilitation of Scapholunate Ligament Instability Following Ganglion Cyst in a Recreational Basketball Player: A Case Report.Cureus. 2024 Aug 30;16(8):e68257. doi: 10.7759/cureus.68257. eCollection 2024 Aug. Cureus. 2024. PMID: 39350849 Free PMC article.
References
-
- Slade J.F., Milewski M.D. Management of carpal instability in athletes. Hand Clin. 2009;25(3):395–408. - PubMed
-
- Tosti R., Shin E. Wrist arthroscopy for athletic injuries. Hand Clin. 2017 Feb;33(1):107–117. - PubMed
-
- Watson H.K., Ballet F.L. The SLAC wrist: scapholunate advanced collapse pattern of degenerative arthritis. J Hand Surg. 1984;9(3):358–365. - PubMed
-
- Beck A. The integrity of the scapholunate ligament in competitive divers. Br J Sports Med. 2019;53(13):843. 1–843.
-
- Benjamin H.J., Engel S.C., Chudzik D. Wrist pain in gymnasts: a review of common overuse wrist pathology in the gymnastics athlete. Curr Sports Med Rep. 2017;16(5):322–329. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
