

Clinical Results of Carpal Tunnel Release Using Ultrasound Guidance in Over 100 Patients at Two to Six Years
- PMID: 38817770
- PMCID: PMC11133916
- DOI: 10.1016/j.jhsg.2024.02.004
Clinical Results of Carpal Tunnel Release Using Ultrasound Guidance in Over 100 Patients at Two to Six Years
Abstract
Purpose: The purpose of this study was to determine the clinical results of carpal tunnel release using ultrasound guidance (CTR-US) at a minimum of 2 years postprocedure.
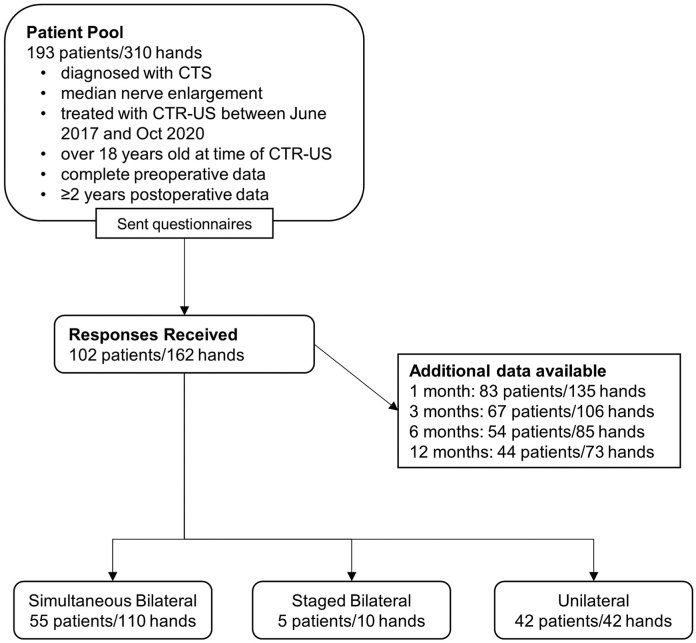
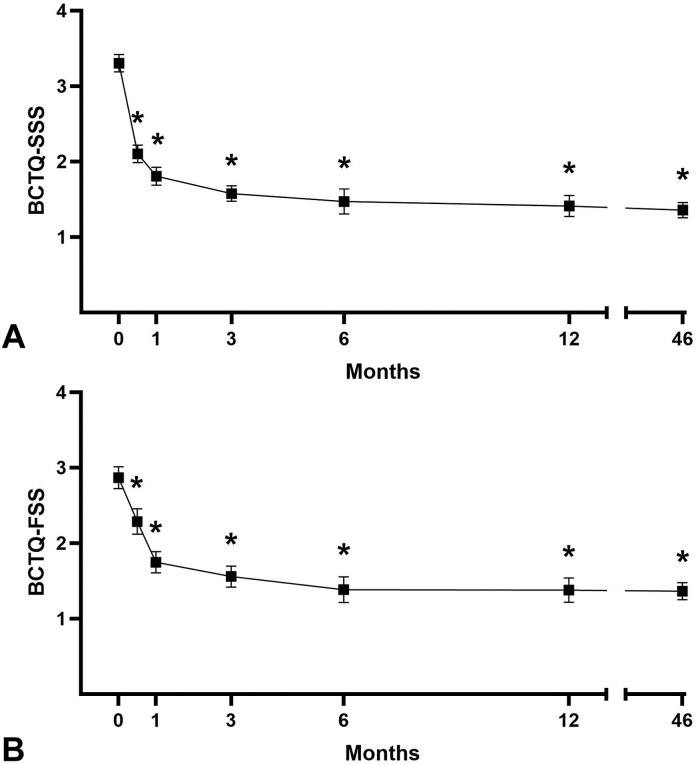
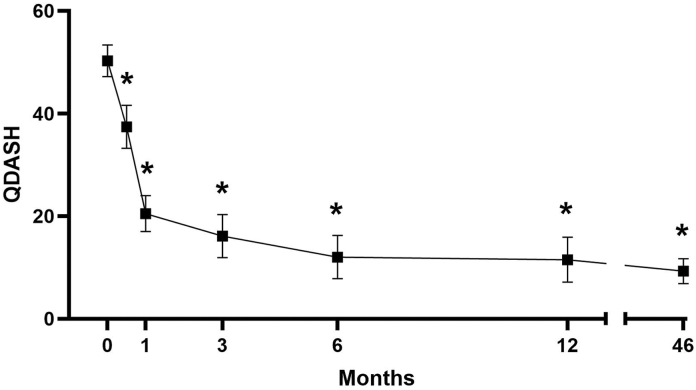
Methods: The study consisted of 102 patients (162 hands) treated with CTR-US by the same physician between June 2017 and October 2020 for whom minimum 2-year follow-up data were available. Questionnaires were sent to gather long-term information, with additional phone calls for clarification if needed. Outcomes included Boston Carpal Tunnel Questionnaire symptom severity (BCTQ-SSS) and functional status (BCTQ-FSS) scores; Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) scores; global satisfaction scores; and subsequent surgeries.
Results: The 102 patients included 68 females and 34 males with a mean age of 56.9 years at the time of surgery. Fifty-five (53.9%) patients had simultaneous bilateral procedures, 42 (41.2%) had unilateral procedures, and 5 (4.9%) had staged bilateral procedures. Significant improvements in BCTQ-SSS, BCTQ-FSS, and QuickDASH scores persisted at a mean final follow-up of 46 months (range 2-6 years). At final follow-up, 91.2% of patients reported satisfaction with the procedure. No outcomes were significantly different between those treated with simultaneous bilateral versus unilateral procedures. No revision surgeries were reported.
Conclusions: CTR-US is a safe and effective procedure that results in significant improvements that persist up to 6 years postprocedure. Long-term results of simultaneous bilateral and unilateral procedures are similar.
Type of study/level of evidence: Therapeutic IV.
Keywords: CTR-US; Carpal tunnel release; Carpal tunnel syndrome; Minimally invasive surgery; Ultrasound.
© 2024 The Authors.
Conflict of interest statement
No benefits in any form have been received or will be received related directly to this article.
Figures
Similar articles
-
Long-term Clinical Results of Carpal Tunnel Release Using Ultrasound Guidance.Hand (N Y). 2022 Nov;17(6):1074-1081. doi: 10.1177/1558944720988080. Epub 2021 Jan 29. Hand (N Y). 2022. PMID: 33511873 Free PMC article.
-
Long-Term Clinical Results of Carpal Tunnel Release Using Ultrasound Guidance: A Multicenter Pragmatic Study.J Hand Surg Glob Online. 2023 Nov 22;6(1):79-84. doi: 10.1016/j.jhsg.2023.10.001. eCollection 2024 Jan. J Hand Surg Glob Online. 2023. PMID: 38313613 Free PMC article.
-
Office-Based Carpal Tunnel Release Using Ultrasound Guidance in a Community Setting: Long-Term Results.Cureus. 2022 Jul 23;14(7):e27169. doi: 10.7759/cureus.27169. eCollection 2022 Jul. Cureus. 2022. PMID: 35898805 Free PMC article.
-
Acupuncture and related interventions for the treatment of symptoms associated with carpal tunnel syndrome.Cochrane Database Syst Rev. 2018 Dec 2;12(12):CD011215. doi: 10.1002/14651858.CD011215.pub2. Cochrane Database Syst Rev. 2018. PMID: 30521680 Free PMC article.
-
Flexor Tenosynovectomy for Recurrent Carpal Tunnel Syndrome: A Retrospective Case Series of 108 Hands.Hand (N Y). 2021 Jan;16(1):18-24. doi: 10.1177/1558944719840735. Epub 2019 Apr 2. Hand (N Y). 2021. PMID: 30939941 Free PMC article. Review.
Cited by
-
Ultrasound-Guided Percutaneous Release and Mini-Open Surgery in Carpal Tunnel Syndrome: A Comparison of Short- and Long-Term Outcomes.Medicina (Kaunas). 2025 Apr 25;61(5):799. doi: 10.3390/medicina61050799. Medicina (Kaunas). 2025. PMID: 40428757 Free PMC article.
References
-
- Atroshi I., Englund M., Turkiewicz A., Tagil M., Petersson I.F. Incidence of physician-diagnosed carpal tunnel syndrome in the general population. Arch Intern Med. 2011;171(10):943–944. - PubMed
-
- Atroshi I., Gummesson C., Johnsson R., Ornstein E., Ranstam J., Rosen I. Prevalence of carpal tunnel syndrome in a general population. JAMA. 1999;282(2):153–158. - PubMed
-
- Sevy JO, Sina RE, Varacallo M. Carpal tunnel syndrome. [Updated 2023 Oct 29]. In: StatPearls [Internet]. 2023. https://www.ncbi.nlm.nih.gov/books/NBK448179/ - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
