

Treatment of unstable forearm fractures at the metaphyseal-diaphyseal junction in children: antegrade ESIN vs. transepiphyseal intramedullary K-wire fixation
- PMID: 38819682
- PMCID: PMC11666750
- DOI: 10.1007/s00068-024-02562-3
Treatment of unstable forearm fractures at the metaphyseal-diaphyseal junction in children: antegrade ESIN vs. transepiphyseal intramedullary K-wire fixation
Abstract
Background: Treatment of unstable forearm fractures in the metaphyseal-diaphyseal junction (MDJ) zone is still a matter of debate. Major drawbacks of all types of fixations include either invasiveness, technical impracticality, or lack of acceptance by patients. This study reports results after antegrade ESIN (a-ESIN) compared to transepiphyseal intramedullary K-wire (TIK) for unstable MDJ forearm fractures.
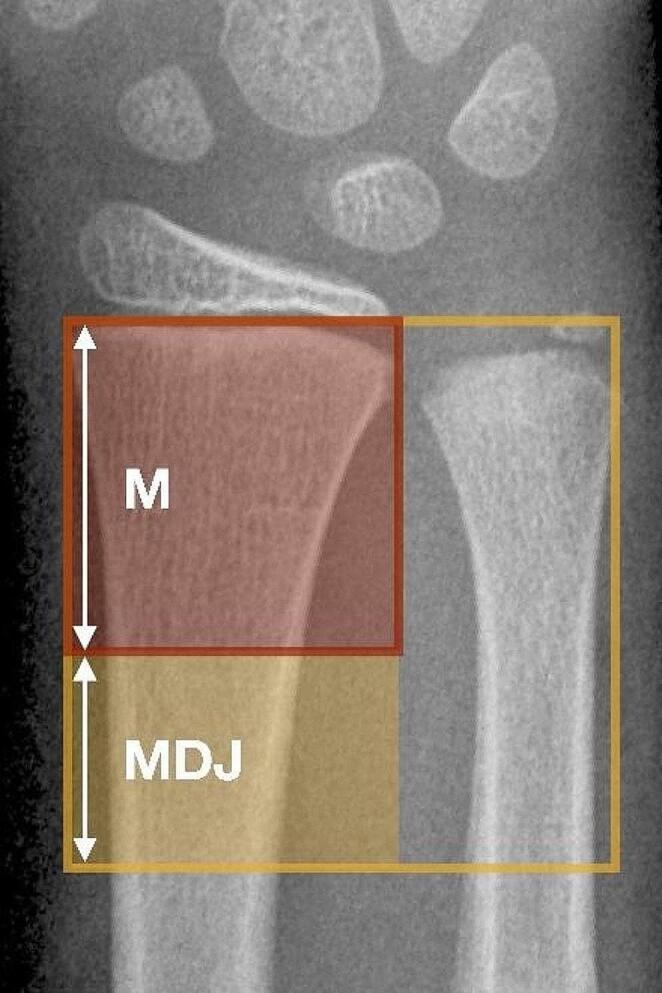
Methods: The MDJ of the forearm was defined as the square over the joints of both forearm bones subtracted with the square over the metaphysis of the radius alone. The data of 40 consecutive patients < 16 years of age who were treated either by a-ESIN (later treatment period) or TIK (early treatment period) for an unstable MDJ forearm fracture at a single high-volume pediatric trauma center were retrospectively analyzed.
Results: The average age was slightly lower in the first group (TIK = 7.42 years; a-ESIN = 10.5 years). An additional ulna fracture was found in 50% of cases and was treated with a classic antegrade ESIN in 10/20 (TIK) and 6/20 cases (a-ESIN). Additional plaster cast immobilization was performed in all cases with TIK and in three cases with a-ESIN. After TIK, no complication, malalignment, or functional limitation occurred. After a-ESIN, 19/20 patients had an event-free course with stable retention and healing without axial malalignment. In one case, a temporary sensor dysfunction occurred. The same patient suffered a refracture two months after the original trauma, which required a closed reduction. Metal removal was performed after 84 days (TIK) and 150 days (a-ESIN). The outcome in all patients was good.
Conclusion: Both a-ESIN and TIK are minimally invasive procedures that are technically easy to perform. Both methods are safe and lead to a complete restoration of the forearm's range of motion. The decisive advantage of a-ESIN is the possibility of postoperative immobilization-free rehabilitation.
Keywords: Antegrade ESIN; Diametaphysis; Elastic stable intramedullary nailing; Forearm fracture; K-wire; Metaphyseal-diaphyseal junction; Pediatric trauma.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical approval: This study was approved by the Ethical Committee of Eberhard Karls University Tübingen (project no. 630/2019BO2). Dr. Markus Dietzel, Dr. Simon Scherer, Dr. Jakob Spogis, Dr. Hans Joachim Kirschner, Prof. Dr. Jörg Fuchs, and Prof. Dr. Justus Lieber have no conflicts of interest or financial ties to disclose. Ethical approval: This study was approved by the Ethical Committee of Eberhard. Karls University Tübingen (project no. 630/2019BO2).
Figures



References
-
- Kraus R, Ploss C, Staub L, Lieber J, Alt V, Weinberg AM, et al. Fractures of Long bones in children and adolescents. Osteo Trauma care. 2006;14:39–44.
-
- Naranje SM, Erali RA, Warner WC Jr., Sawyer JR, Kelly DM. Epidemiology of Pediatric fractures presenting to Emergency Departments in the United States. J Pediatr Orthop. 2016;36(4):e45–8. 10.1097/BPO.0000000000000595. - PubMed
-
- Lascombes P, Haumont T, Journeau P. Use and abuse of flexible intramedullary nailing in children and adolescents. J Pediatr Orthop. 2006;26(6):827–34. 10.1097/01.bpo.0000235397.64783.d6. - PubMed
-
- Sinikumpu JJ, Nietosvaara Y. Treatment of distal forearm fractures in children. Scand J Surg. 2021;110(2):276–80. 10.1177/1457496920983104. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
