

ACKR3 Antagonism Enhances the Repair of Demyelinated Lesions Through Both Immunomodulatory and Remyelinating Effects
- PMID: 38819698
- PMCID: PMC11233362
- DOI: 10.1007/s11064-024-04173-1
ACKR3 Antagonism Enhances the Repair of Demyelinated Lesions Through Both Immunomodulatory and Remyelinating Effects
Abstract
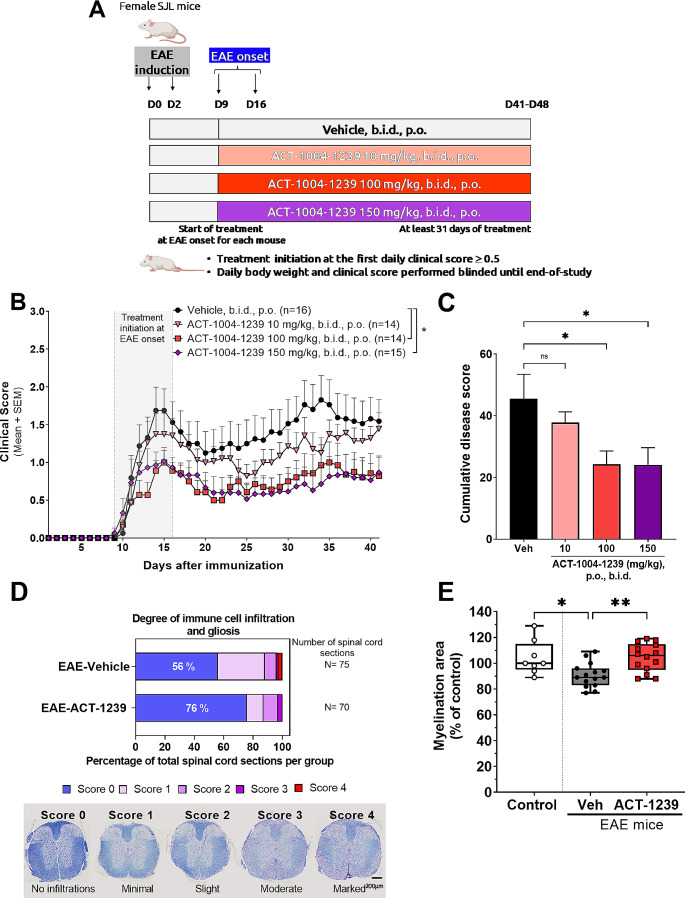
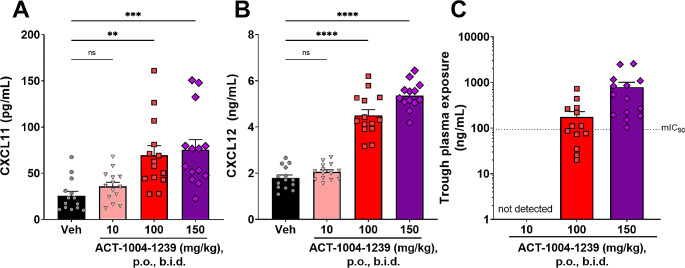
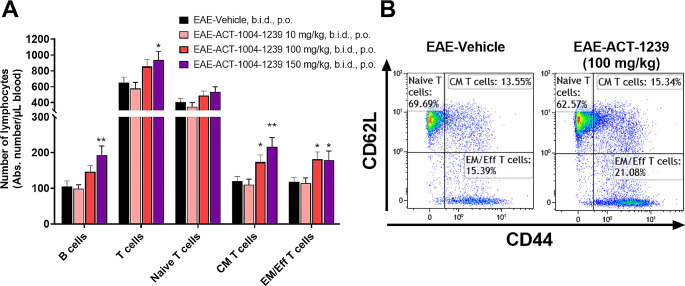
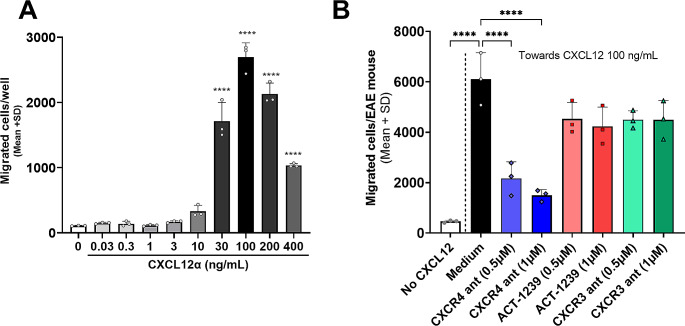
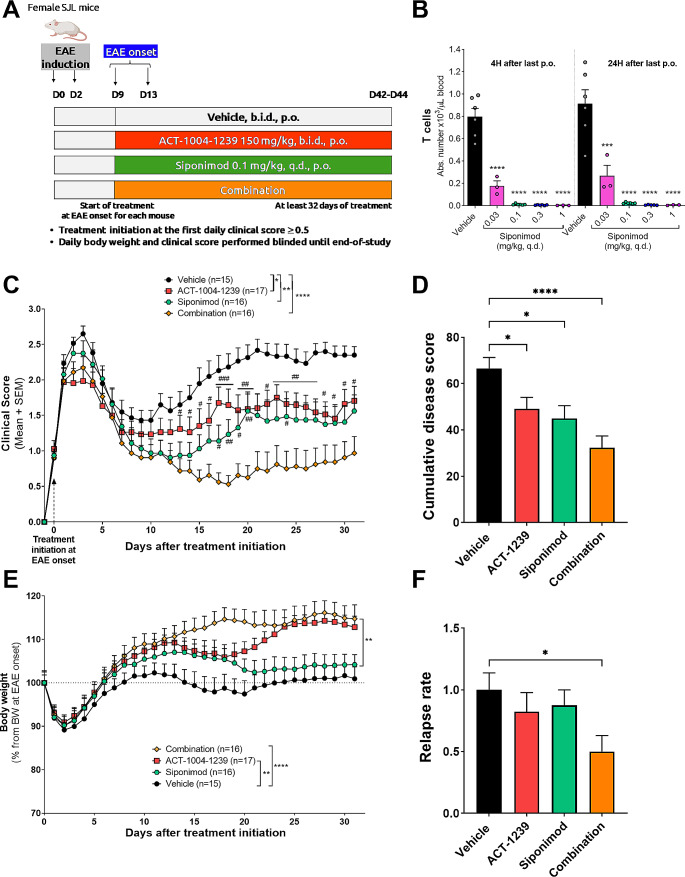
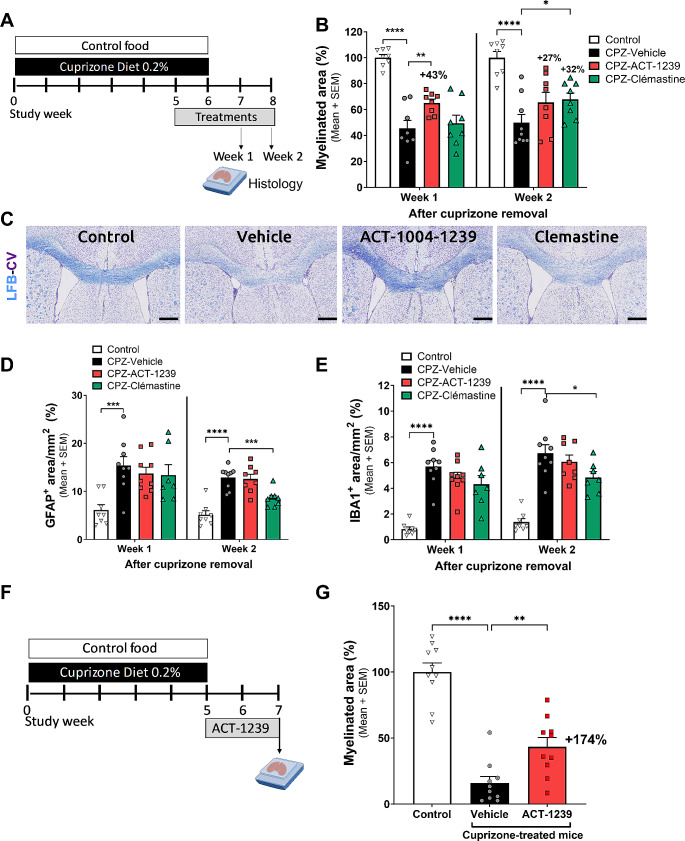
Addressing inflammation, demyelination, and associated neurodegeneration in inflammatory demyelinating diseases like multiple sclerosis (MS) remains challenging. ACT-1004-1239, a first-in-class and potent ACKR3 antagonist, currently undergoing clinical development, showed promise in preclinical MS models, reducing neuroinflammation and demyelination. However, its effectiveness in treating established disease and impact on remyelination after the occurrence of demyelinated lesions remain unexplored. This study assessed the therapeutic effect of ACT-1004-1239 in two demyelinating disease models. In the proteolipid protein (PLP)-induced experimental autoimmune encephalomyelitis (EAE) model, ACT-1004-1239 administered upon the detection of the first signs of paralysis, resulted in a dose-dependent reduction in EAE disease severity, concomitant with diminished immune cell infiltrates in the CNS and reduced demyelination. Notably, efficacy correlated with elevated plasma concentrations of CXCL11 and CXCL12, two pharmacodynamic biomarkers of ACKR3 antagonism. Combining ACT-1004-1239 with siponimod, an approved immunomodulatory treatment for MS, synergistically reduced EAE severity. In the cuprizone-induced demyelination model, ACT-1004-1239 administered after 5 weeks of cuprizone exposure, significantly accelerated remyelination, already quantifiable one week after cuprizone withdrawal. Additionally, ACT-1004-1239 penetrated the CNS, elevating brain CXCL12 concentrations. These results demonstrate that ACKR3 antagonism significantly reduces the severity of experimental demyelinating diseases, even when treatment is initiated therapeutically, after the occurrence of lesions. It confirms the dual mode of action of ACT-1004-1239, exhibiting both immunomodulatory effects by reducing neuroinflammation and promyelinating effects by accelerating myelin repair. The results further strengthen the rationale for evaluating ACT-1004-1239 in clinical trials for patients with demyelinating diseases.
Keywords: ACKR3/CXCR7; CXCL11; CXCL12; Immunomodulation; Multiple sclerosis; Remyelination.
© 2024. The Author(s).
Conflict of interest statement
All the authors acknowledge that the work was performed as employees of Idorsia Pharmaceuticals Ltd. The authors declare no other financial interests.
Figures


Similar articles
-
ACT-1004-1239, a first-in-class CXCR7 antagonist with both immunomodulatory and promyelinating effects for the treatment of inflammatory demyelinating diseases.FASEB J. 2021 Mar;35(3):e21431. doi: 10.1096/fj.202002465R. FASEB J. 2021. PMID: 33595155 Free PMC article.
-
Siponimod supports remyelination in the non-supportive environment.Sci Rep. 2025 Feb 4;15(1):4216. doi: 10.1038/s41598-025-87825-8. Sci Rep. 2025. PMID: 39905182 Free PMC article.
-
Myelin repair is accelerated by inactivating CXCR2 on nonhematopoietic cells.J Neurosci. 2010 Jul 7;30(27):9074-83. doi: 10.1523/JNEUROSCI.1238-10.2010. J Neurosci. 2010. PMID: 20610741 Free PMC article.
-
Nudging oligodendrocyte intrinsic signaling to remyelinate and repair: Estrogen receptor ligand effects.J Steroid Biochem Mol Biol. 2016 Jun;160:43-52. doi: 10.1016/j.jsbmb.2016.01.006. Epub 2016 Jan 14. J Steroid Biochem Mol Biol. 2016. PMID: 26776441 Free PMC article. Review.
-
De- and remyelination in the CNS white and grey matter induced by cuprizone: the old, the new, and the unexpected.Histol Histopathol. 2011 Dec;26(12):1585-97. doi: 10.14670/HH-26.1585. Histol Histopathol. 2011. PMID: 21972097 Review.
References
-
- Plemel JR, Liu W-Q, Yong VW. Remyelination therapies: a new direction and challenge in multiple sclerosis. Nat Rev Drug Discovery. 2017;16(9):617–634. - PubMed
-
- Chu T, Shields LBE, Zhang YP, Feng SQ, Shields CB, Cai J. CXCL12/CXCR4/CXCR7 Chemokine Axis in the Central Nervous System: therapeutic targets for Remyelination in Demyelinating diseases. Neuroscientist. 2017;23(6):627–648. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
