

Inferior vena cava distensibility during pressure support ventilation: a prospective study evaluating interchangeability of subcostal and trans‑hepatic views, with both M‑mode and automatic border tracing
- PMID: 38819726
- PMCID: PMC11427491
- DOI: 10.1007/s10877-024-01177-8
Inferior vena cava distensibility during pressure support ventilation: a prospective study evaluating interchangeability of subcostal and trans‑hepatic views, with both M‑mode and automatic border tracing
Abstract
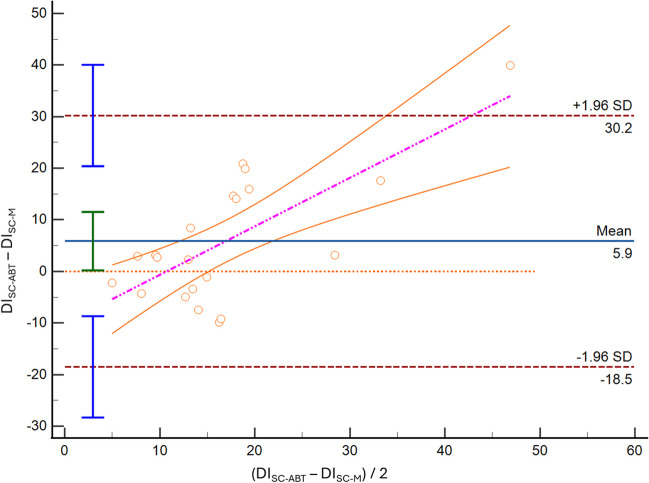
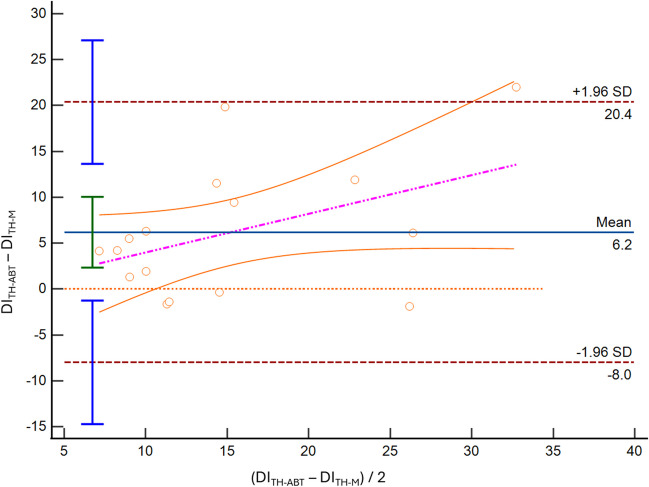
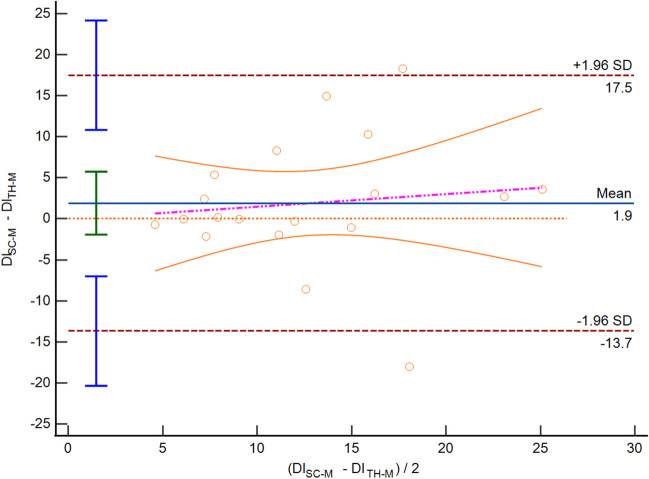
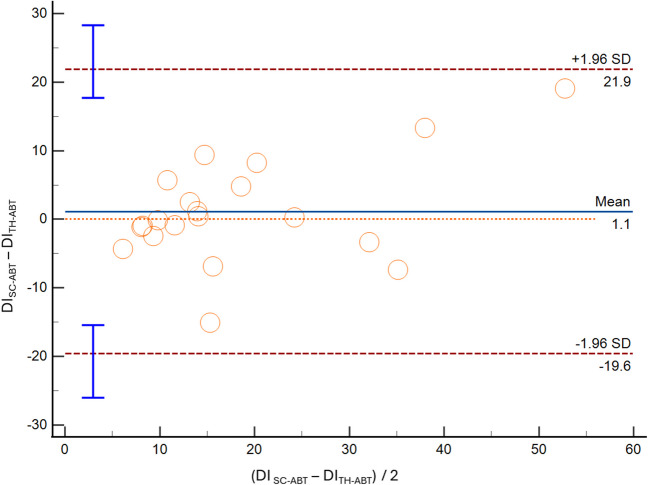
The Inferior Vena Cava (IVC) is commonly utilized to evaluate fluid status in the Intensive Care Unit (ICU),with more recent emphasis on the study of venous congestion. It is predominantly measured via subcostal approach (SC) or trans-hepatic (TH) views, and automated border tracking (ABT) software has been introduced to facilitate its assessment. Prospective observational study on patients ventilated in pressure support ventilation (PSV) with 2 × 2 factorial design. Primary outcome was to evaluate interchangeability of measurements of the IVC and the distensibility index (DI) obtained using both M-mode and ABT, across both SC and TH. Statistical analyses comprised Bland-Altman assessments for mean bias, limits of agreement (LoA), and the Spearman correlation coefficients. IVC visualization was 100% successful via SC, while TH view was unattainable in 17.4% of cases. As compared to the M-mode, the IVC-DI obtained through ABT approach showed divergences in both SC (mean bias 5.9%, LoA -18.4% to 30.2%, ICC = 0.52) and TH window (mean bias 6.2%, LoA -8.0% to 20.4%, ICC = 0.67). When comparing the IVC-DI measures obtained in the two anatomical sites, accuracy improved with a mean bias of 1.9% (M-mode) and 1.1% (ABT), but LoA remained wide (M-mode: -13.7% to 17.5%; AI: -19.6% to 21.9%). Correlation was generally suboptimal (r = 0.43 to 0.60). In PSV ventilated patients, we found that IVC-DI calculated with M-mode is not interchangeable with ABT measurements. Moreover, the IVC-DI gathered from SC or TH view produces not comparable results, mainly in terms of precision.
Keywords: Artificial intelligence; Correlation; Echocardiography; Fluid responsiveness; Vexus.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Inferior vena cava distensibility from subcostal and trans-hepatic imaging using both M-mode or artificial intelligence: a prospective study on mechanically ventilated patients.Intensive Care Med Exp. 2023 Jul 10;11(1):40. doi: 10.1186/s40635-023-00529-z. Intensive Care Med Exp. 2023. PMID: 37423948 Free PMC article.
-
Assessment of the inferior vena cava collapsibility from subcostal and trans-hepatic imaging using both M-mode or artificial intelligence: a prospective study on healthy volunteers.Intensive Care Med Exp. 2023 Apr 3;11(1):15. doi: 10.1186/s40635-023-00505-7. Intensive Care Med Exp. 2023. PMID: 37009935 Free PMC article.
-
Subcostal versus transhepatic view to assess the inferior vena cava in critically ill patients.Echocardiography. 2020 Aug;37(8):1171-1176. doi: 10.1111/echo.14802. Epub 2020 Aug 5. Echocardiography. 2020. PMID: 32757463
-
Accuracy of Ultrasonographic Measurements of Inferior Vena Cava to Determine Fluid Responsiveness: A Systematic Review and Meta-Analysis.J Intensive Care Med. 2020 Apr;35(4):354-363. doi: 10.1177/0885066617752308. Epub 2018 Jan 17. J Intensive Care Med. 2020. PMID: 29343170
-
Assessment of fluid responsiveness using pulse pressure variation, stroke volume variation, plethysmographic variability index, central venous pressure, and inferior vena cava variation in patients undergoing mechanical ventilation: a systematic review and meta-analysis.Crit Care. 2024 Aug 31;28(1):289. doi: 10.1186/s13054-024-05078-9. Crit Care. 2024. PMID: 39217370 Free PMC article.
Cited by
-
Understanding the Brain-Heart-Lung Triangle: Mission Impossible?Neurocrit Care. 2025 Feb;42(1):310-311. doi: 10.1007/s12028-024-02109-9. Epub 2024 Sep 5. Neurocrit Care. 2025. PMID: 39237843 No abstract available.
References
-
- Via G, Tavazzi G, Price S. Ten situations where inferior vena cava ultrasound may fail to accurately predict fluid responsiveness: a physiologically based point of view. Intensive Care Med. 2016;42:1164–7. - PubMed
-
- Vignon P, Repesse X, Begot E, Leger J, Jacob C, Bouferrache K, Slama M, Prat G, Vieillard-Baron A. Comparison of echocardiographic indices used to predict fluid responsiveness in ventilated patients. Am J Respir Crit Care Med. 2017;195:1022–32. - PubMed
-
- Sanfilippo F, Messina A, Cecconi M, Astuto M. Ten answers to key questions for fluid management in intensive care. Med Intensiva. 2021;45(9):552–62. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
