

Incidence of self-reported tuberculosis treatment with community-wide universal testing and treatment for HIV and tuberculosis screening in Zambia and South Africa: A planned analysis of the HPTN 071 (PopART) cluster-randomised trial
- PMID: 38820246
- PMCID: PMC11142425
- DOI: 10.1371/journal.pmed.1004393
Incidence of self-reported tuberculosis treatment with community-wide universal testing and treatment for HIV and tuberculosis screening in Zambia and South Africa: A planned analysis of the HPTN 071 (PopART) cluster-randomised trial
Abstract
Background: HIV is a potent risk factor for tuberculosis (TB). Therefore, community-wide universal testing and treatment for HIV (UTT) could contribute to TB control, but evidence for this is limited. Community-wide TB screening can decrease population-level TB prevalence. Combining UTT with TB screening could therefore significantly impact TB control in sub-Saharan Africa, but to our knowledge there is no evidence for this combined approach.
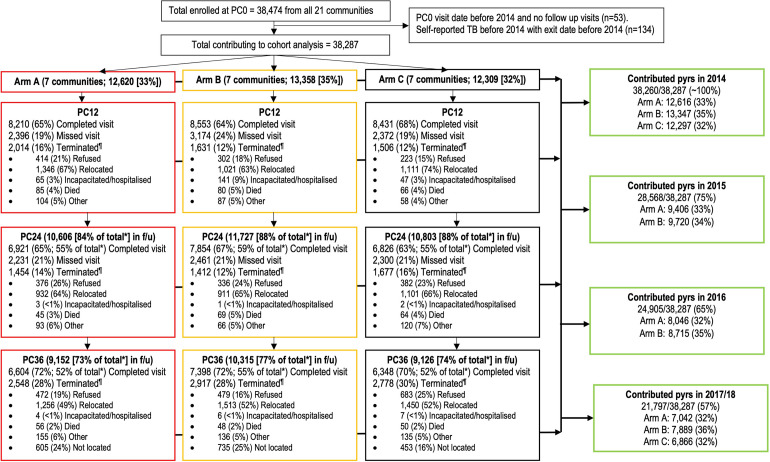
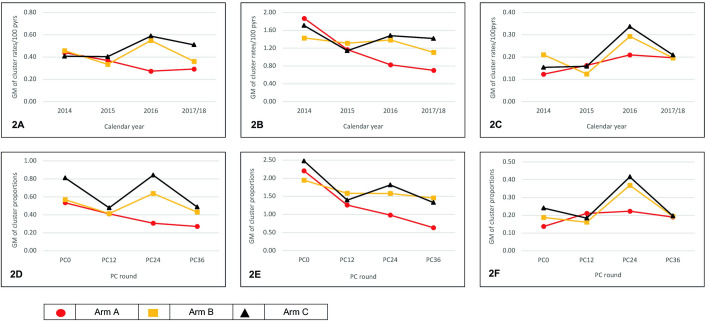
Methods and findings: HPTN 071 (PopART) was a community-randomised trial conducted between November 2013 to July 2018; 21 Zambian and South African communities (with a total population of approximately 1 million individuals) were randomised to arms A (community-wide UTT and TB screening), B (community-wide universal HIV testing with treatment following national guidelines and TB screening), or C (standard-of-care). In a cohort of randomly selected adults (18 to 44 years) enrolled between 2013 and 2015 from all 21 communities (total size 38,474; 27,139 [71%] female; 8,004 [21%] HIV positive) and followed-up annually for 36 months to measure the population-level impact of the interventions, data on self-reported TB treatment in the previous 12 months (self-reported TB) were collected by trained research assistants and recorded using a structured questionnaire at each study visit. In this prespecified analysis of the trial, self-reported TB incidence rates were measured by calendar year between 2014 and 2017/2018. A p-value ≤0.05 on hypothesis testing was defined as reaching statistical significance. Between January 2014 and July 2018, 38,287 individuals were followed-up: 494 self-reported TB during 104,877 person-years. Overall incidence rates were similar across all arms in 2014 and 2015 (0.33 to 0.46/100 person-years). In 2016 incidence rates were lower in arm A compared to C overall (adjusted rate ratio [aRR] 0.48 [95% confidence interval (95% CI) 0.28 to 0.81; p = 0.01]), with statistical significance reached. In 2017/2018, while incidence rates were lower in arm A compared to C, statistical significance was not reached (aRR 0.58 [95% CI 0.27 to 1.22; p = 0.13]). Among people living with HIV (PLHIV) incidence rates were lower in arm A compared to C in 2016 (RR 0.56 [95% CI 0.29 to 1.08; p = 0.08]) and 2017/2018 (RR 0.50 [95% CI 0.26 to 0.95; p = 0.04]); statistical significance was only reached in 2017/2018. Incidence rates in arms B and C were similar, overall and among PLHIV. Among HIV-negative individuals, there were too few events for cross-arm comparisons. Study limitations include the use of self-report which may have been subject to under-reporting, limited covariate adjustment due to the small number of events, and high losses to follow-up over time.
Conclusions: In this study, community-wide UTT and TB screening resulted in substantially lower TB incidence among PLHIV at population-level, compared to standard-of-care, with statistical significance reached in the final study year. There was also some evidence this translated to a decrease in self-reported TB incidence overall in the population. Reduction in arm A but not B suggests UTT drove the observed effect. Our data support the role of UTT in TB control, in addition to HIV control, in high TB/HIV burden settings.
Trial registration: ClinicalTrials.gov: NCT01900977.
Copyright: © 2024 Telisinghe et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Tuberculosis prevalence after 4 years of population-wide systematic TB symptom screening and universal testing and treatment for HIV in the HPTN 071 (PopART) community-randomised trial in Zambia and South Africa: A cross-sectional survey (TREATS).PLoS Med. 2023 Sep 8;20(9):e1004278. doi: 10.1371/journal.pmed.1004278. eCollection 2023 Sep. PLoS Med. 2023. PMID: 37682971 Free PMC article. Clinical Trial.
-
HPTN 071 (PopART): rationale and design of a cluster-randomised trial of the population impact of an HIV combination prevention intervention including universal testing and treatment - a study protocol for a cluster randomised trial.Trials. 2014 Feb 13;15:57. doi: 10.1186/1745-6215-15-57. Trials. 2014. PMID: 24524229 Free PMC article. Clinical Trial.
-
Impact of universal testing and treatment on sexual risk behaviour and herpes simplex virus type 2: a prespecified secondary outcomes analysis of the HPTN 071 (PopART) community-randomised trial.Lancet HIV. 2022 Nov;9(11):e760-e770. doi: 10.1016/S2352-3018(22)00253-3. Lancet HIV. 2022. PMID: 36332653 Free PMC article. Clinical Trial.
-
Achieving the UNAIDS 90-90-90 targets: a comparative analysis of four large community randomised trials delivering universal testing and treatment to reduce HIV transmission in sub-Saharan Africa.BMC Public Health. 2022 Dec 13;22(1):2333. doi: 10.1186/s12889-022-14713-5. BMC Public Health. 2022. PMID: 36514036 Free PMC article.
-
Integrating and Interpreting Findings from the Latest Treatment as Prevention Trials.Curr HIV/AIDS Rep. 2020 Jun;17(3):249-258. doi: 10.1007/s11904-020-00492-4. Curr HIV/AIDS Rep. 2020. PMID: 32297219 Free PMC article. Review.
References
-
- World Health Organization. Global tuberculosis report 2022. Available from: https://www.who.int/publications/i/item/9789240061729; accessed 2023 Jan 14.
-
- World Health Organization. Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV 2015. Available from: https://www.who.int/publications/i/item/9789241509565; accessed 2023 Jan 14. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
