

Heme-induced loss of renovascular endothelial protein C receptor promotes chronic kidney disease in sickle mice
- PMID: 38820589
- PMCID: PMC11307268
- DOI: 10.1182/blood.2023023528
Heme-induced loss of renovascular endothelial protein C receptor promotes chronic kidney disease in sickle mice
Abstract
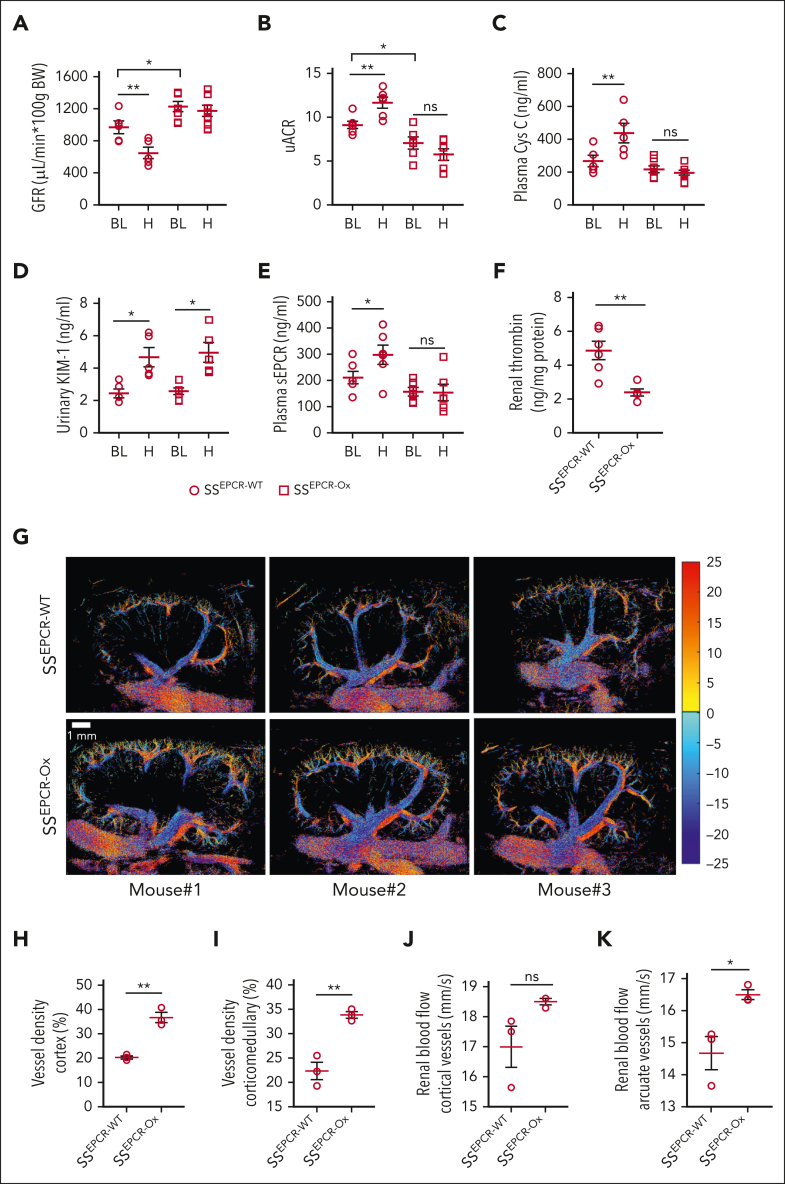
Chronic kidney disease (CKD) is a major contributor to morbidity and mortality in sickle cell disease (SCD). Anemia, induced by chronic persistent hemolysis, is associated with the progressive deterioration of renal health, resulting in CKD. Moreover, patients with SCD experience acute kidney injury (AKI), a risk factor for CKD, often during vaso-occlusive crisis associated with acute intravascular hemolysis. However, the mechanisms of hemolysis-driven pathogenesis of the AKI-to-CKD transition in SCD remain elusive. Here, we investigated the role of increased renovascular rarefaction and the resulting substantial loss of the vascular endothelial protein C receptor (EPCR) in the progressive deterioration of renal function in transgenic SCD mice. Multiple hemolytic events raised circulating levels of soluble EPCR (sEPCR), indicating loss of EPCR from the cell surface. Using bone marrow transplantation and super-resolution ultrasound imaging, we demonstrated that SCD mice overexpressing EPCR were protective against heme-induced CKD development. In a cohort of patients with SCD, plasma sEPCR was significantly higher in individuals with CKD than in those without CKD. This study concludes that multiple hemolytic events may trigger CKD in SCD through the gradual loss of renovascular EPCR. Thus, the restoration of EPCR may be a therapeutic target, and plasma sEPCR can be developed as a prognostic marker for sickle CKD.
© 2024 American Society of Hematology. Published by Elsevier Inc. All rights are reserved, including those for text and data mining, AI training, and similar technologies.
Conflict of interest statement
Conflict-of-interest disclosure: S.G. receives research funding (not relevant to the present study) from Pfizer Inc as part of a sponsored research agreement. The remaining authors declare no competing financial interests.
Figures







Comment in
-
EPCR shedding light on sickle nephropathy.Blood. 2024 Aug 1;144(5):472-474. doi: 10.1182/blood.2024025479. Blood. 2024. PMID: 39088231 Free PMC article. No abstract available.
Similar articles
-
Sickle Cell Disease.2003 Sep 15 [updated 2025 Feb 13]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. 2003 Sep 15 [updated 2025 Feb 13]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993–2025. PMID: 20301551 Free Books & Documents. Review.
-
Interventions for chronic kidney disease in people with sickle cell disease.Cochrane Database Syst Rev. 2023 Aug 4;8(8):CD012380. doi: 10.1002/14651858.CD012380.pub3. Cochrane Database Syst Rev. 2023. PMID: 37539955 Free PMC article.
-
Hydroxyurea (hydroxycarbamide) for sickle cell disease.Cochrane Database Syst Rev. 2022 Sep 1;9(9):CD002202. doi: 10.1002/14651858.CD002202.pub3. Cochrane Database Syst Rev. 2022. PMID: 36047926 Free PMC article.
-
Taurodeoxycholic acid impairs the function and expression of organic anion transporter 2 through farnesoid X receptor activation during acute kidney injury to chronic kidney injury transition.Drug Metab Dispos. 2025 Jul;53(7):100097. doi: 10.1016/j.dmd.2025.100097. Epub 2025 May 13. Drug Metab Dispos. 2025. PMID: 40513229
-
Interventions for chronic kidney disease in people with sickle cell disease.Cochrane Database Syst Rev. 2017 Jul 3;7(7):CD012380. doi: 10.1002/14651858.CD012380.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2023 Aug 4;8:CD012380. doi: 10.1002/14651858.CD012380.pub3. PMID: 28672087 Free PMC article. Updated.
Cited by
-
EPCR shedding light on sickle nephropathy.Blood. 2024 Aug 1;144(5):472-474. doi: 10.1182/blood.2024025479. Blood. 2024. PMID: 39088231 Free PMC article. No abstract available.
-
Nitrated fatty acids protect against acute kidney injury in sickle cell disease.Blood Adv. 2025 Jun 24;9(12):2886-2890. doi: 10.1182/bloodadvances.2024015038. Blood Adv. 2025. PMID: 40117493 Free PMC article.
-
The APC-EPCR-PAR1 axis in sickle cell disease.Front Med (Lausanne). 2023 Jul 11;10:1141020. doi: 10.3389/fmed.2023.1141020. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37497271 Free PMC article. Review.
References
-
- Gosmanova EO, Zaidi S, Wan JY, Adams-Graves PE. Prevalence and progression of chronic kidney disease in adult patients with sickle cell disease. J Investig Med. 2014;62(5):804–807. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
