

Lymphatic failure and lymphatic interventions: Knowledge gaps and future directions for a new frontier in congenital heart disease
- PMID: 38820801
- PMCID: PMC11229519
- DOI: 10.1016/j.sempedsurg.2024.151426
Lymphatic failure and lymphatic interventions: Knowledge gaps and future directions for a new frontier in congenital heart disease
Abstract
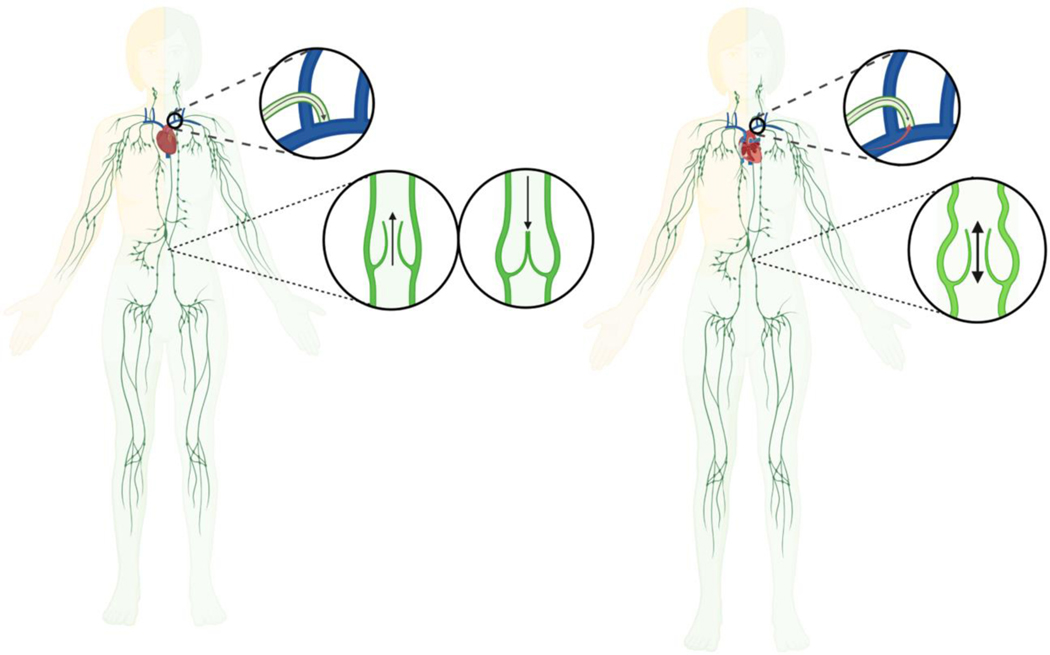
Lymphatic failure is a broad term that describes the lymphatic circulation's inability to adequately transport fluid and solutes out of the interstitium and into the systemic venous circulation, which can result in dysfunction and dysregulation of immune responses, dietary fat absorption, and fluid balance maintenance. Several investigations have recently elucidated the nexus between lymphatic failure and congenital heart disease, and the associated morbidity and mortality is now well-recognized. However, the precise pathophysiology and pathogenesis of lymphatic failure remains poorly understood and relatively understudied, and there are no targeted therapeutics or interventions to reliably prevent its development and progression. Thus, there is growing enthusiasm towards the development and application of novel percutaneous and surgical lymphatic interventions. Moreover, there is consensus that further investigations are needed to delineate the underlying mechanisms of lymphatic failure, which could help identify novel therapeutic targets and develop innovative procedures to improve the overall quality of life and survival of these patients. With these considerations, this review aims to provide an overview of the lymphatic circulation and its vasculature as it relates to current understandings into the pathophysiology and pathogenesis of lymphatic failure in patients with congenital heart disease, while also summarizing strategies for evaluating and managing lymphatic complications, as well as specific areas of interest for future translational and clinical research efforts.
Copyright © 2024 Elsevier Inc. All rights reserved.
Figures




References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
