

Robotic versus laparoscopic distal gastrectomy for resectable gastric cancer: a randomized phase 2 trial
- PMID: 38821945
- PMCID: PMC11143299
- DOI: 10.1038/s41467-024-49013-6
Robotic versus laparoscopic distal gastrectomy for resectable gastric cancer: a randomized phase 2 trial
Abstract
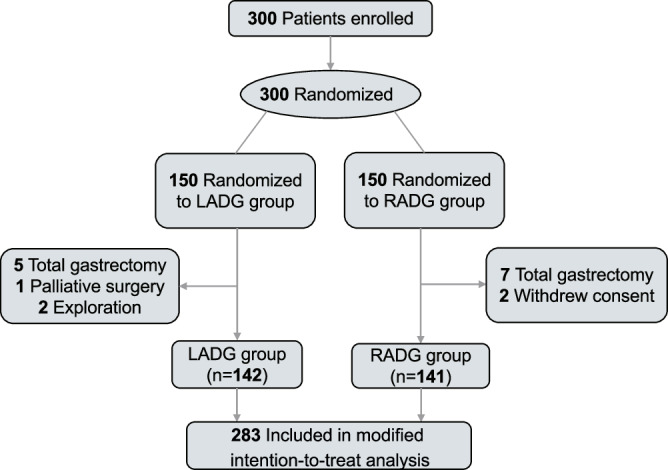
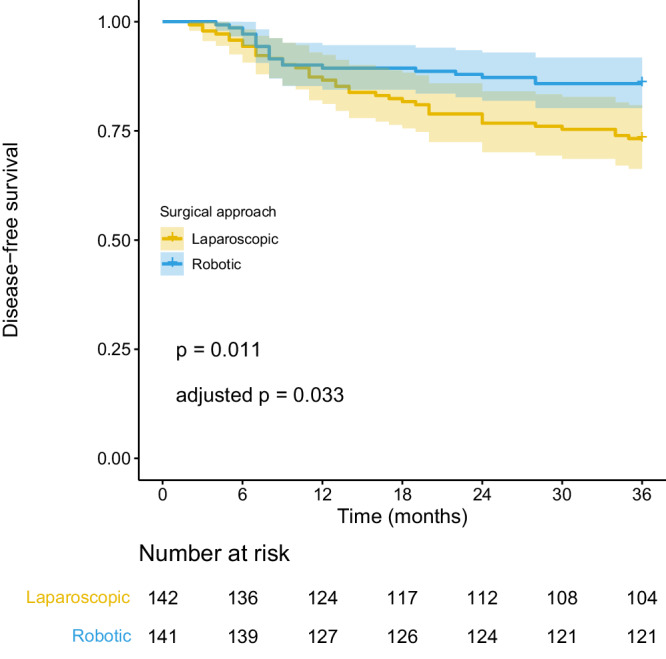
Robotic surgery may be an alternative to laparoscopic surgery for gastric cancer (GC). However, randomized controlled trials (RCTs) reporting the differences in survival between these two approaches are currently lacking. From September 2017 to January 2020, 300 patients with cT1-4a and N0/+ were enrolled and randomized to either the robotic (RDG) or laparoscopic distal gastrectomy (LDG) group (NCT03313700). The primary endpoint was 3-year disease-free survival (DFS); secondary endpoints reported here are the 3-year overall survival (OS) and recurrence patterns. The remaining secondary outcomes include intraoperative outcomes, postoperative recovery, quality of lymphadenectomy, and cost differences, which have previously been reported. There were 283 patients in the modified intention-to-treat analysis (RDG group: n = 141; LDG group: n = 142). The trial has met pre-specified endpoints. The 3-year DFS rates were 85.8% and 73.2% in the RDG and LDG groups, respectively (p = 0.011). Multivariable Cox regression model including age, tumor size, sex, ECOG PS, lymphovascular invasion, histology, pT stage, and pN stage showed that RDG was associated with better 3-year DFS (HR: 0.541; 95% CI: 0.314-0.932). The RDG also improved the 3-year cumulative recurrence rate (RDG vs. LDG: 12.1% vs. 21.1%; HR: 0.546, 95% CI: 0.302-0.990). Compared to LDG, RDG demonstrated non-inferiority in 3-year DFS rate.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Assessment of Robotic Versus Laparoscopic Distal Gastrectomy for Gastric Cancer: A Randomized Controlled Trial.Ann Surg. 2021 May 1;273(5):858-867. doi: 10.1097/SLA.0000000000004466. Ann Surg. 2021. PMID: 32889876 Clinical Trial.
-
Comparison of robotic versus laparoscopic versus open distal gastrectomy for locally advanced gastric cancer: a prospective trial-based economic evaluation.Surg Endosc. 2023 Oct;37(10):7472-7485. doi: 10.1007/s00464-023-10147-1. Epub 2023 Jul 3. Surg Endosc. 2023. PMID: 37395806
-
Comparison of Surgical Outcomes Between Robotic and Laparoscopic Distal Gastrectomy for cT1 Gastric Cancer.World J Surg. 2018 Jun;42(6):1803-1810. doi: 10.1007/s00268-017-4345-4. World J Surg. 2018. PMID: 29134310
-
Establishing the Learning Curve of Laparoscopic and Robotic Distal Gastrectomy: a Systematic Review and Meta-Regression Analysis.J Gastrointest Surg. 2023 Dec;27(12):2946-2982. doi: 10.1007/s11605-023-05812-8. Epub 2023 Sep 1. J Gastrointest Surg. 2023. PMID: 37658172
-
Laparoscopic versus open distal gastrectomy for advanced gastric cancer: A meta-analysis of randomized controlled trials and high-quality nonrandomized comparative studies.Eur J Surg Oncol. 2020 Nov;46(11):1998-2010. doi: 10.1016/j.ejso.2020.06.046. Epub 2020 Jul 11. Eur J Surg Oncol. 2020. PMID: 32758382 Review.
Cited by
-
Laparoscopic vs robot-assisted gastrectomy in gastric cancer patients with prior abdominal surgery: a propensity-matched analysis.J Robot Surg. 2025 May 4;19(1):196. doi: 10.1007/s11701-025-02347-9. J Robot Surg. 2025. PMID: 40319425
-
Machine learning assisted radiomics in predicting postoperative occurrence of deep venous thrombosis in patients with gastric cancer.BMC Cancer. 2025 Feb 7;25(1):220. doi: 10.1186/s12885-025-13630-1. BMC Cancer. 2025. PMID: 39920636 Free PMC article.
-
Short- and long-term outcomes of robotic- versus laparoscopic-assisted early-onset gastric cancer: a propensity score-matched retrospective cohort study.BMC Cancer. 2025 Feb 27;25(1):361. doi: 10.1186/s12885-025-13767-z. BMC Cancer. 2025. PMID: 40016662 Free PMC article.
-
Transcriptional landscape and predictive potential of long noncoding RNAs in peritoneal recurrence of gastric cancer.Mol Cancer. 2024 Dec 30;23(1):284. doi: 10.1186/s12943-024-02196-4. Mol Cancer. 2024. PMID: 39736670 Free PMC article.
-
Modern Management of Common Bile Duct Stones: Breakthroughs, Challenges, and Future Perspectives.Cureus. 2024 Dec 6;16(12):e75246. doi: 10.7759/cureus.75246. eCollection 2024 Dec. Cureus. 2024. PMID: 39776736 Free PMC article. Review.
References
-
- Kitano S, et al. Laparoscopy-assisted Billroth I gastrectomy. Surg. Laparosc. Endosc. 1994;4:146–148. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
