

Intermittent blood flow restriction with low-load resistance training for older adults with knee osteoarthritis: a randomized, controlled, non-inferiority trial protocol
- PMID: 38822360
- PMCID: PMC11140873
- DOI: 10.1186/s13063-024-08203-9
Intermittent blood flow restriction with low-load resistance training for older adults with knee osteoarthritis: a randomized, controlled, non-inferiority trial protocol
Abstract
Background: Knee osteoarthritis (KOA) is a chronic musculoskeletal disorder characterized by pain and functional impairment. Blood flow restriction (BFR) with low-load resistance training (LLRT) demonstrates a similar improvement in clinical outcomes to high-load resistance training (HLRT) in treating KOA. It has not been established whether intermittent blood flow restriction (iBFR) with LLRT can lead to clinical outcomes that are comparable to those produced by continuous blood flow restriction (cBFR) with LLRT and HLRT. The aim of the proposed study is to evaluate the efficacy of iBFR with LLRT on pain, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), muscle strength, muscle mass, physical function, perceptions of discomfort and effort, and adherence in KOA patients.
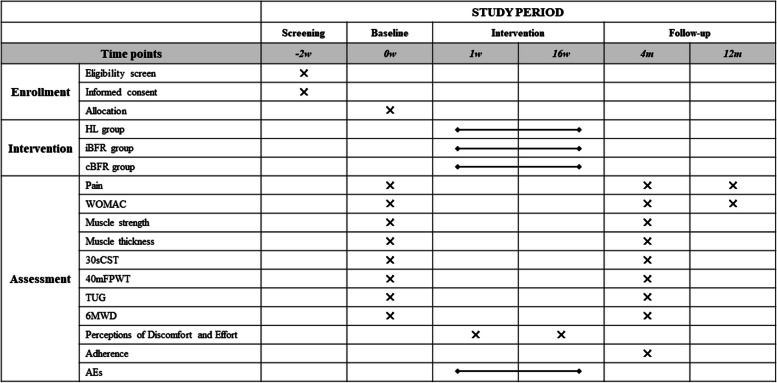
Methods: This is a three-arm, non-inferiority, randomized controlled trial utilizing blinded assessors. Two hundred thirteen participants will be randomly allocated to one of the following three groups: iBFR group-receiving 4 months of LLRT with iBFR, twice weekly (n = 71); cBFR group-receiving 4 months of LLRT with cBFR, twice weekly (n = 71); or HLRT group-receiving 4 months of HLRT without BFR, twice weekly (n = 71). The primary outcome is pain. The secondary outcomes include the WOMAC, muscle strength, muscle mass, physical function, perceptions of discomfort and effort, and adherence. Pain and WOMAC will be measured at the baseline and 4 and 12 months after randomizations. Muscle strength, muscle mass, and physical function will be measured at the baseline and 4 months after randomizations. The perceptions of discomfort and effort will be measured during the first and final sessions.
Discussion: BFR with LLRT has a similar improvement in clinical outcomes as HLRT. However, cBFR may cause elevated ratings of perceived exertion and local discomfort, compromising patient tolerability and treatment adherence. If iBFR with LLRT could produce improvement in clinical outcomes analogous to those of HLRT and iBFR with LLRT, it could be considered an alternative approach for treating patients with KOA.
Trial registration: Chinese Clinical Trial Registry ChiCTR2300072820. Registered on June 26, 2023.
Keywords: Blood flow restriction; Knee osteoarthritis; Rehabilitation; Resistance training; Vascular occlusion.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

Similar articles
-
Effect of low-load resistance training with different degrees of blood flow restriction in patients with knee osteoarthritis: study protocol for a randomized trial.Trials. 2022 Jan 3;23(1):6. doi: 10.1186/s13063-021-05946-7. Trials. 2022. PMID: 34980197 Free PMC article.
-
Blood flow restriction with different load levels in patients with knee osteoarthritis: protocol of a randomized controlled trial.Trials. 2022 Jan 15;23(1):41. doi: 10.1186/s13063-022-05998-3. Trials. 2022. PMID: 35033169 Free PMC article.
-
Effects of blood flow restriction exercise with very low load and low volume in patients with knee osteoarthritis: protocol for a randomized trial.Trials. 2019 Feb 18;20(1):135. doi: 10.1186/s13063-019-3238-2. Trials. 2019. PMID: 30777115 Free PMC article.
-
Acute effects of resistance exercise with blood flow restriction on cardiovascular response: a meta-analysis.J Comp Eff Res. 2022 Aug;11(11):829-842. doi: 10.2217/cer-2021-0272. Epub 2022 Jun 17. J Comp Eff Res. 2022. PMID: 35712965 Review.
-
A meta-analysis of randomized controlled trials: evaluating the efficacy of isokinetic muscle strengthening training in improving knee osteoarthritis outcomes.J Orthop Surg Res. 2025 Jan 24;20(1):95. doi: 10.1186/s13018-025-05495-8. J Orthop Surg Res. 2025. PMID: 39856723 Free PMC article.
Cited by
-
Impact of low-load blood flow restriction training on knee osteoarthritis pain and muscle strength: a systematic review and meta-analysis of randomized controlled trials.Front Physiol. 2025 Mar 17;16:1524480. doi: 10.3389/fphys.2025.1524480. eCollection 2025. Front Physiol. 2025. PMID: 40166718 Free PMC article.
References
-
- Dillon CF, Rasch EK, Gu Q, Hirsch R. Prevalence of knee osteoarthritis in the United States: arthritis data from the Third National Health and Nutrition Examination Survey 1991–94. J Rheumatol. 2006;33:2271–2279. - PubMed
-
- Hochberg MC, Altman RD, April KT, Benkhalti M, Guyatt G, McGowan J, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res. 2012;64:465–474. doi: 10.1002/acr.21596. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
