

Ebola virus-induced eye sequelae: a murine model for evaluating glycoprotein-targeting therapeutics
- PMID: 38823088
- PMCID: PMC11169960
- DOI: 10.1016/j.ebiom.2024.105170
Ebola virus-induced eye sequelae: a murine model for evaluating glycoprotein-targeting therapeutics
Abstract
Background: Ebola virus disease (EVD) survivors experience ocular sequelae including retinal lesions, cataracts, and vision loss. While monoclonal antibodies targeting the Ebola virus glycoprotein (EBOV-GP) have shown promise in improving prognosis, their effectiveness in mitigating ocular sequelae remains uncertain.
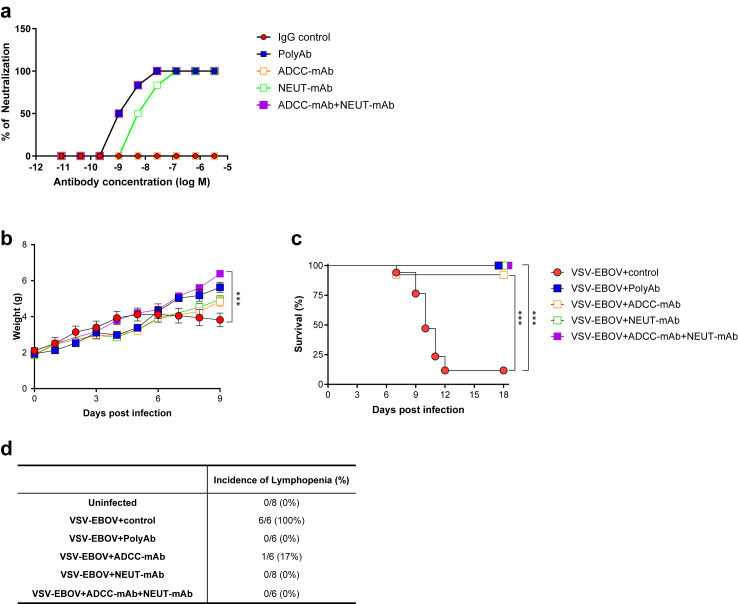
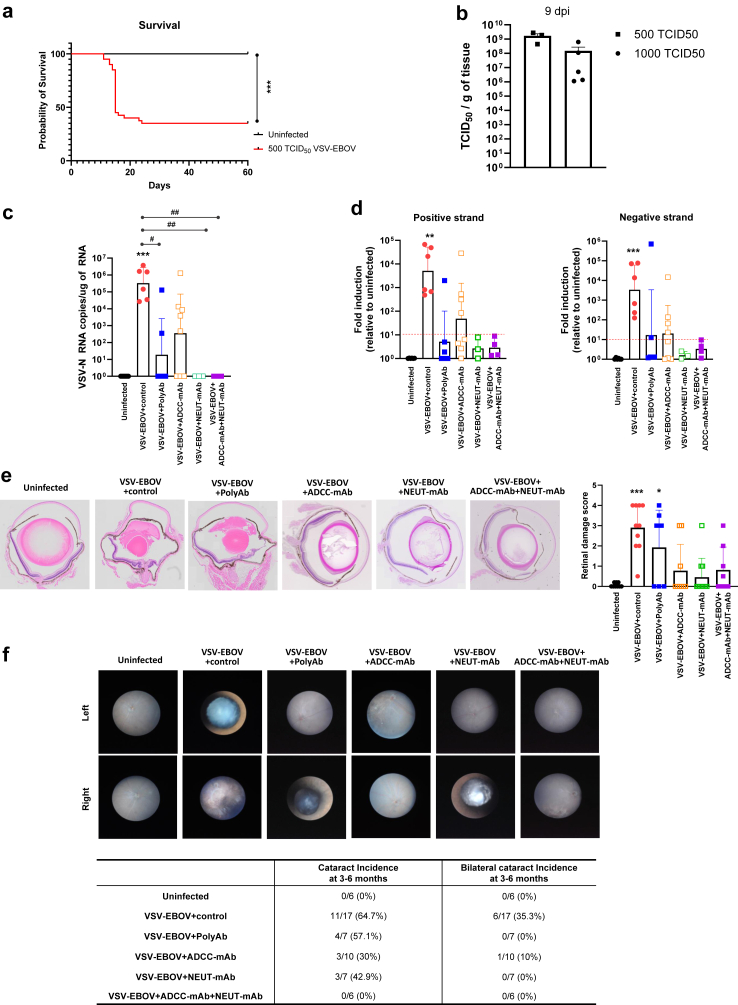
Methods: We developed and characterized a BSL-2-compatible immunocompetent mouse model to evaluate therapeutics targeting EBOV-GP by inoculating neonatal mice with vesicular stomatitis virus expressing EBOV-GP (VSV-EBOV). To examine the impact of anti-EBOV-GP antibody treatment on acute retinitis and ocular sequelae, VSV-EBOV-infected mice were treated with polyclonal antibodies or monoclonal antibody preparations with antibody-dependent cellular cytotoxicity (ADCC-mAb) or neutralizing activity (NEUT-mAb).
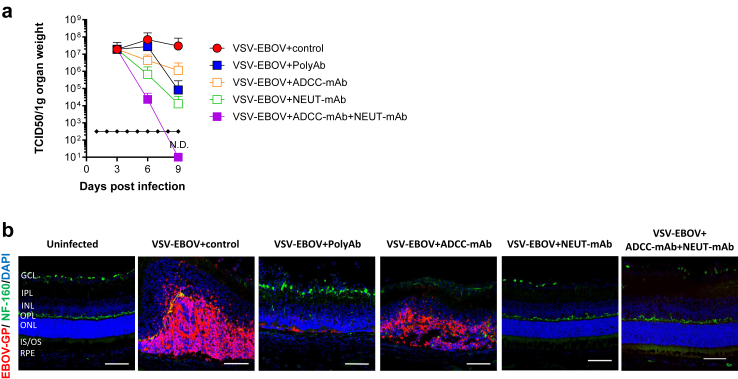
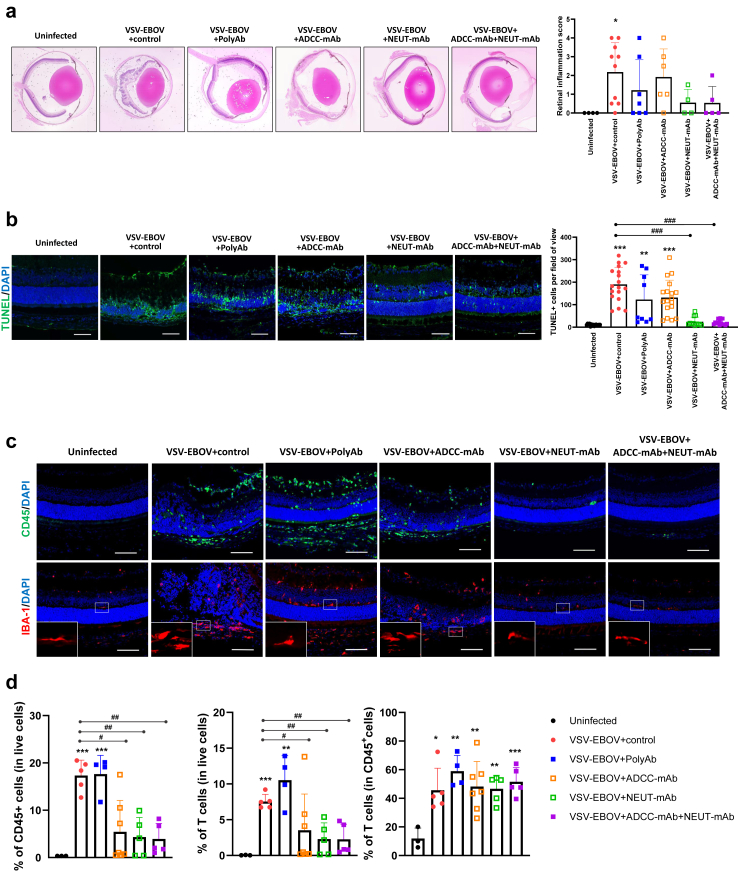
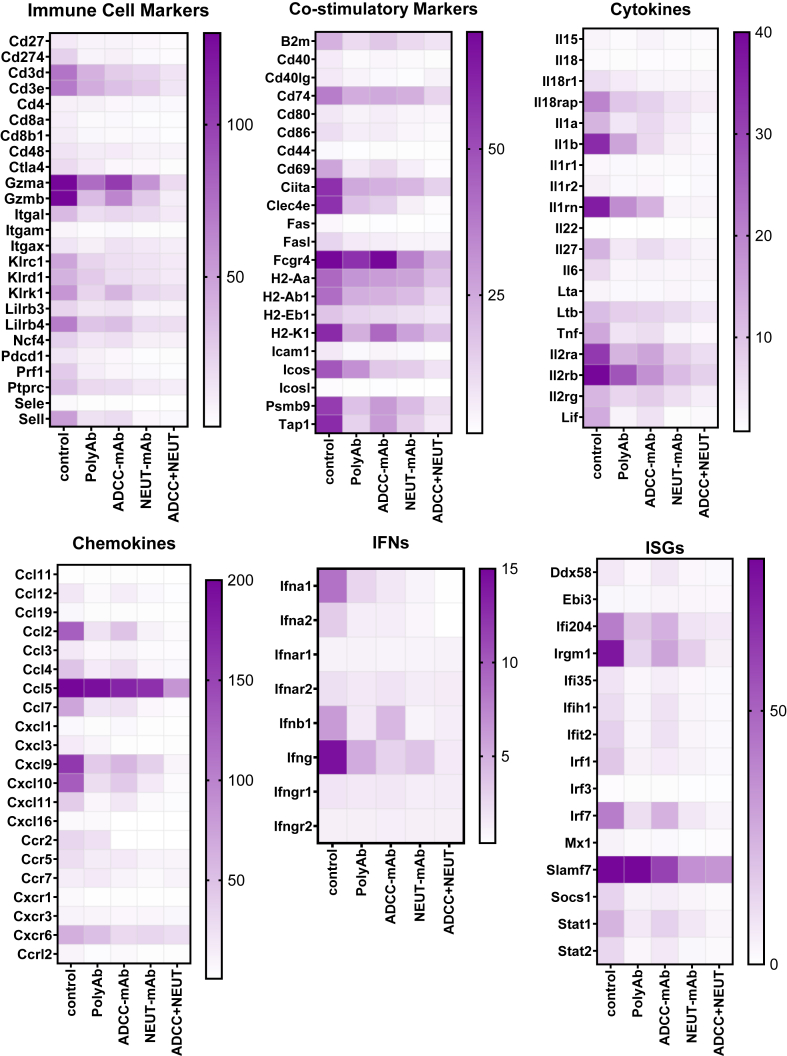
Findings: Treatment with all anti-EBOV-GP antibodies tested dramatically reduced viremia and improved survival. Further, all treatments reduced the incidence of cataracts. However, NEUT-mAb alone or in combination with ADCC-mAb reduced viral load in the eyes, downregulated the ocular immune and inflammatory responses, and minimized retinal damage more effectively.
Interpretation: Anti-EBOV-GP antibodies can improve survival among EVD patients, but improved therapeutics are needed to reduce life altering sequelae. This animal model offers a new platform to examine the acute and long-term effect of the virus in the eye and the relative impact of therapeutic candidates targeting EBOV-GP. Results indicate that even antibodies that improve systemic viral clearance and survival can differ in their capacity to reduce acute ocular inflammation, and long-term retinal pathology and corneal degeneration.
Funding: This study was partly supported by Postgraduate Research Fellowship Awards from ORISE through an interagency agreement between the US DOE and the US FDA.
Keywords: Anti-EBOV-GP antibodies; BSL-2 model; EBOV glycoprotein (EBOV-GP); EBOV-GP pseudotyped vesicular stomatitis virus (VSV-EBOV); Ebola virus (EBOV); Ocular sequelae; Retinitis.
Published by Elsevier B.V.
Conflict of interest statement
Declaration of interests All authors have read and confirmed the manuscript and accepted the responsibility to submit it for publication. The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Characterization of the therapeutic effect of antibodies targeting the Ebola glycoprotein using a novel BSL2-compliant rVSVΔG-EBOV-GP infection model.Emerg Microbes Infect. 2021 Dec;10(1):2076-2089. doi: 10.1080/22221751.2021.1997075. Emerg Microbes Infect. 2021. PMID: 34674613 Free PMC article.
-
High degree of correlation between Ebola virus BSL-4 neutralization assays and pseudotyped VSV BSL-2 fluorescence reduction neutralization test.J Virol Methods. 2018 Apr;254:1-7. doi: 10.1016/j.jviromet.2018.01.003. Epub 2018 Jan 31. J Virol Methods. 2018. PMID: 29355585 Free PMC article.
-
Ebolavirus Glycoprotein Fc Fusion Protein Protects Guinea Pigs against Lethal Challenge.PLoS One. 2016 Sep 13;11(9):e0162446. doi: 10.1371/journal.pone.0162446. eCollection 2016. PLoS One. 2016. PMID: 27622456 Free PMC article.
-
[Research progress on ebola virus glycoprotein].Bing Du Xue Bao. 2013 Mar;29(2):233-7. Bing Du Xue Bao. 2013. PMID: 23757858 Review. Chinese.
-
The Roles of Ebola Virus Soluble Glycoprotein in Replication, Pathogenesis, and Countermeasure Development.Viruses. 2019 Oct 31;11(11):999. doi: 10.3390/v11110999. Viruses. 2019. PMID: 31683550 Free PMC article. Review.
Cited by
-
Long-term Sequelae in Ebola Virus Disease Survivors Receiving Anti-Ebola Virus Therapies in the Democratic Republic of the Congo: A Prospective Cohort Study.Open Forum Infect Dis. 2025 Jul 31;12(8):ofaf436. doi: 10.1093/ofid/ofaf436. eCollection 2025 Aug. Open Forum Infect Dis. 2025. PMID: 40809394 Free PMC article.
References
-
- Murray M.J. Ebola virus disease: a review of its past and present. Anesth Analg. 2015;121(3):798–809. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
