

Preliminary report of a thoracic duct-to-pulmonary vein lymphovenous anastomosis in swine: A novel technique and potential treatment for lymphatic failure
- PMID: 38823193
- PMCID: PMC11265529
- DOI: 10.1016/j.sempedsurg.2024.151427
Preliminary report of a thoracic duct-to-pulmonary vein lymphovenous anastomosis in swine: A novel technique and potential treatment for lymphatic failure
Abstract
Objective: The thoracic duct is the largest lymphatic vessel in the body, and carries fluid and nutrients absorbed in abdominal organs to the central venous circulation. Thoracic duct obstruction can cause significant failure of the lymphatic circulation (i.e., protein-losing enteropathy, plastic bronchitis, etc.). Surgical anastomosis between the thoracic duct and central venous circulation has been used to treat thoracic duct obstruction but cannot provide lymphatic decompression in patients with superior vena cava obstruction or chronically elevated central venous pressures (e.g., right heart failure, single ventricle physiology, etc.). Therefore, this preclinical feasibility study sought to develop a novel and optimal surgical technique for creating a thoracic duct-to-pulmonary vein lymphovenous anastomosis (LVA) in swine that could remain patent and preserve unidirectional lymphatic fluid flow into the systemic venous circulation to provide therapeutic decompression of the lymphatic circulation even at high central venous pressures.
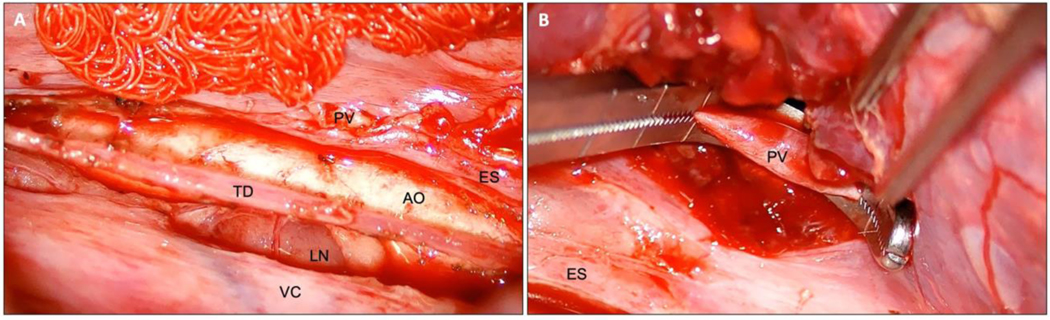
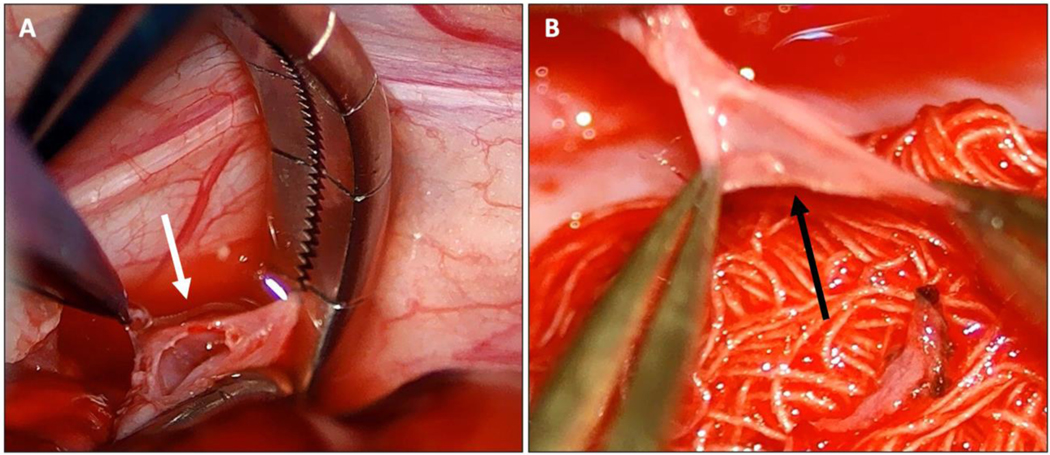
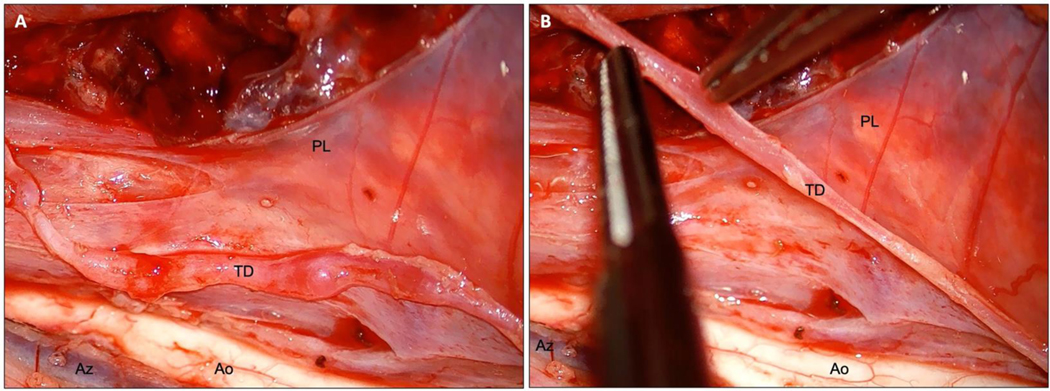
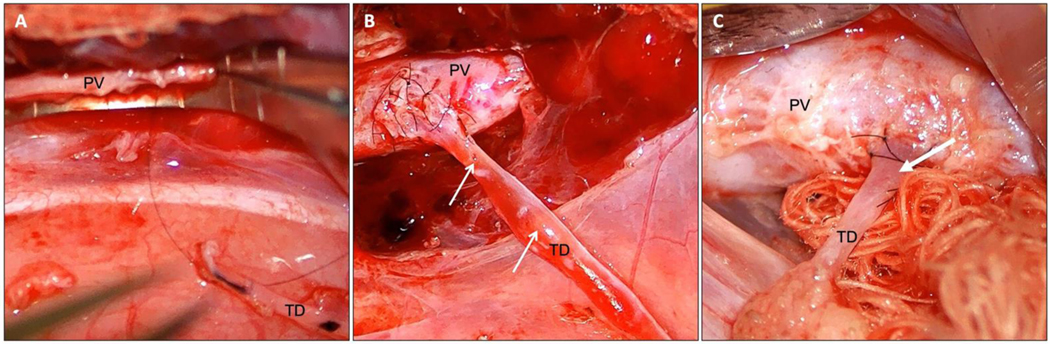
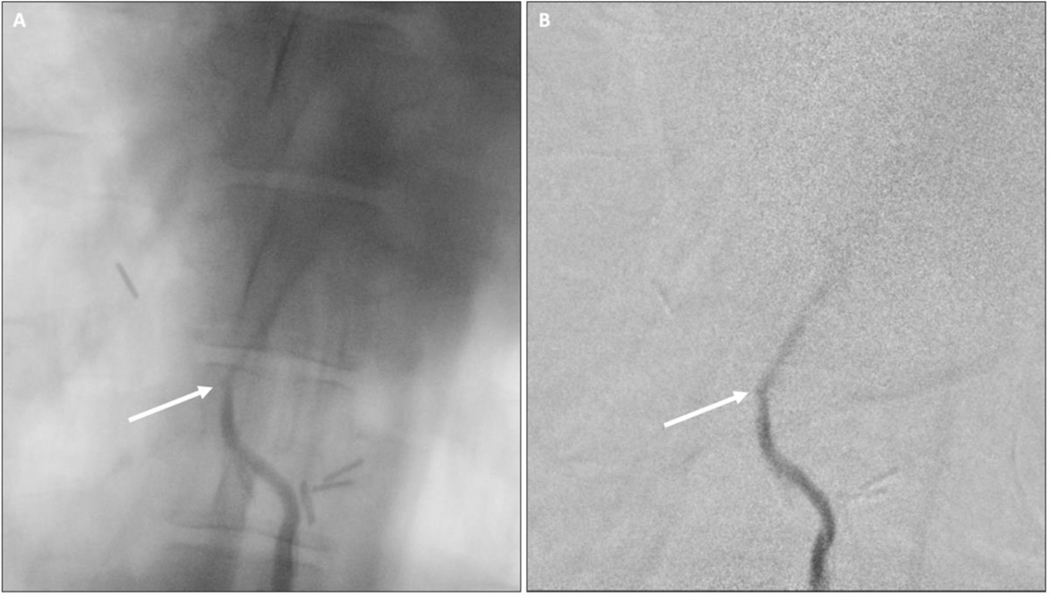
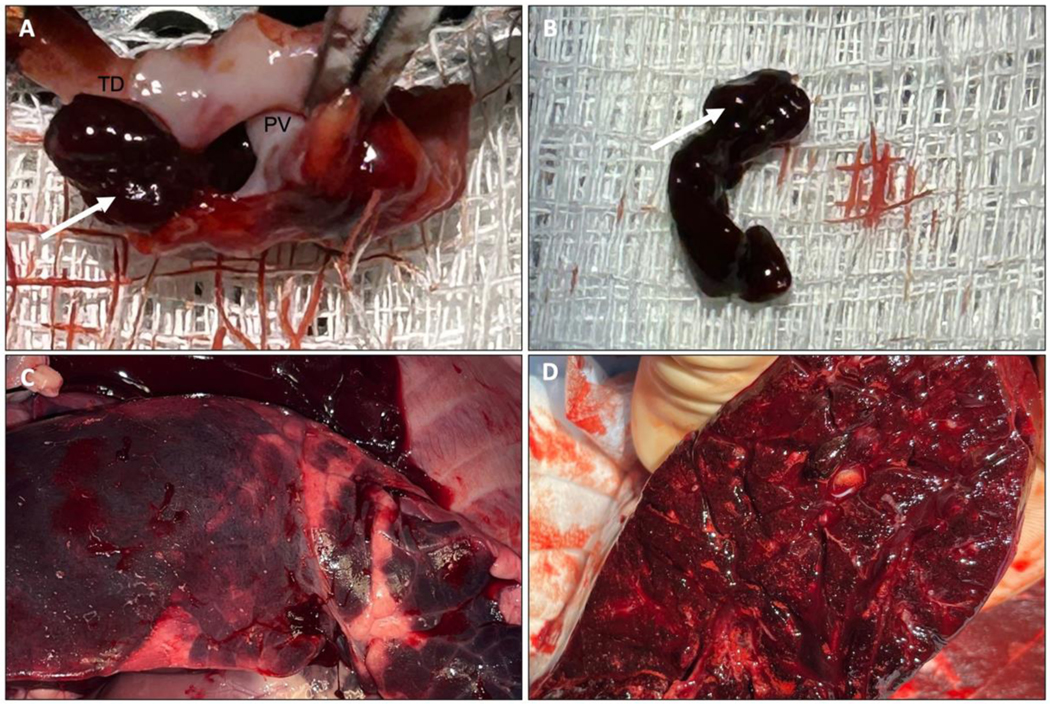
Methods: A thoracic duct-to-pulmonary vein LVA was attempted in 10 piglets (median age 80 [IQR 80-83] days; weight 22.5 [IQR 21.4-26.8] kg). After a right thoracotomy, the thoracic duct was mobilized, transected, and anastomosed to the right inferior pulmonary vein. Animals were systemically anticoagulated on post-operative day 1. Lymphangiography was used to evaluate LVA patency up to post-operative day 7.
Results: A thoracic duct-to-pulmonary vein LVA was successfully completed in 8/10 (80.0%) piglets, of which 6/8 (75.0%) survived to the intended study endpoint without any complication (median 6 [IQR 4-7] days). Initially, 2/10 (20.0%) LVAs were aborted intraoperatively, and 2/10 (20.0%) animals were euthanized early due to post-operative complications. However, using an optimized surgical technique, the success rate for creating a thoracic duct-to-pulmonary vein LVA in six animals was 100%, all of which survived to their intended study endpoint without any complications (median 6 [IQR 4-7] days). LVAs remained patent for up to seven days.
Conclusion: A thoracic duct-to-pulmonary vein LVA can be completed safely and remain patent for at least one week with systemic anticoagulation, which provides an important proof-of-concept that this novel intervention could effectively offload the lymphatic circulation in patients with lymphatic failure and elevated central venous pressures.
Keywords: Congenital heart disease; Fontan procedure; Lymphatic failure; Lymphatic flow disorder; Lympho-venous anastomosis; Lymphovenous anastomosis.
Copyright © 2024 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Anesthetic challenges in patients with multicompartmental lymphatic failure after Fontan palliation undergoing transcatheter thoracic duct decompression.Paediatr Anaesth. 2024 Jul;34(7):597-601. doi: 10.1111/pan.14891. Epub 2024 Apr 23. Paediatr Anaesth. 2024. PMID: 38651655
-
Proposal for Prevention or Alleviation of Protein/Lymph-Losing Enteropathy (PLE/LLE) After Fontan Circulation Treatment of Univentricular Hearts: Restoration of Lymph Balance With a "Lymphatic Right-to-Left Shunt.".Lymphology. 2016 Sep;49(3):114-27. Lymphology. 2016. PMID: 29906066
-
The Deciding Factors of Flow Direction in Lymphovenous Anastomosis for Extremity Lymphedema.Plast Reconstr Surg. 2023 Dec 1;152(6):1350-1357. doi: 10.1097/PRS.0000000000010865. Epub 2023 Jun 20. Plast Reconstr Surg. 2023. PMID: 37337319
-
Current diagnostic and therapeutic strategies for the management of lymphatic insufficiency in patients with hypoplastic left heart syndrome.Front Pediatr. 2023 Feb 24;11:1058567. doi: 10.3389/fped.2023.1058567. eCollection 2023. Front Pediatr. 2023. PMID: 36911024 Free PMC article. Review.
-
Lymphovenous anastomosis (LVA) for treatment of secondary breast lymphedema: A case report and literature review.Microsurgery. 2021 Feb;41(2):165-169. doi: 10.1002/micr.30629. Epub 2020 Jul 17. Microsurgery. 2021. PMID: 32678929 Review.
References
-
- Fudim M, Salah HM, Sathananthan J, Bernier M, Pabon-Ramos W, Schwartz RS, Rodés-Cabau J, Côté F, Khalifa A, Virani SA, Patel MR. Lymphatic Dysregulation in Patients With Heart Failure: JACC Review Topic of the Week. J Am Coll Cardiol. 2021;78(1):66–76. - PubMed
-
- Itkin M, Rockson SG, Burkhoff D. Pathophysiology of the Lymphatic System in Patients With Heart Failure: JACC State-of-the-Art Review. J Am Coll Cardiol. 2021;78(3):278–290. - PubMed
-
- Rychik J, Atz AM, Celermajer DS, Deal BJ, Gatzoulis MA, Gewillig MH, Hsia TY, Hsu DT, Kovacs AH, McCrindle BW, Newburger JW, Pike NA, Rodefeld M, Rosenthal DN, Schumacher KR, Marino BS, Stout K, Veldtman G, Younoszai AK, d’Udekem Y; American Heart Association Council on Cardiovascular Disease in the Young and Council on Cardiovascular and Stroke Nursing. Evaluation and Management of the Child and Adult With Fontan Circulation: A Scientific Statement From the American Heart Association. Circulation. 2019;140(6):e234–e284. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
