

Inhibition of lysine acetyltransferase KAT6 in ER+HER2- metastatic breast cancer: a phase 1 trial
- PMID: 38824244
- PMCID: PMC11333285
- DOI: 10.1038/s41591-024-03060-0
Inhibition of lysine acetyltransferase KAT6 in ER+HER2- metastatic breast cancer: a phase 1 trial
Erratum in
-
Author Correction: Inhibition of lysine acetyltransferase KAT6 in ER+HER2- metastatic breast cancer: a phase 1 trial.Nat Med. 2024 Aug;30(8):2371. doi: 10.1038/s41591-024-03129-w. Nat Med. 2024. PMID: 38914862 Free PMC article. No abstract available.
Abstract
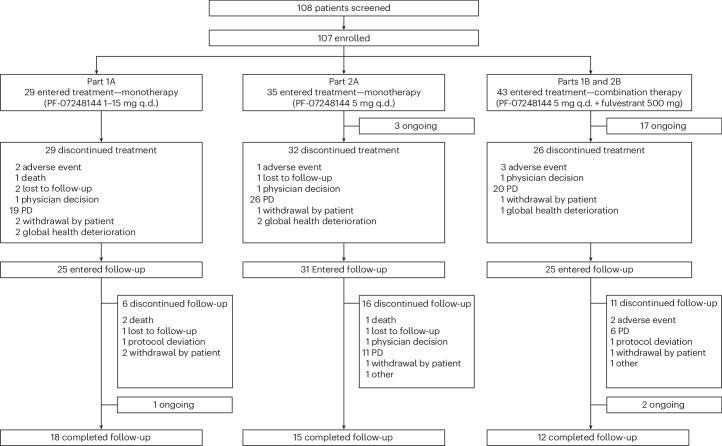
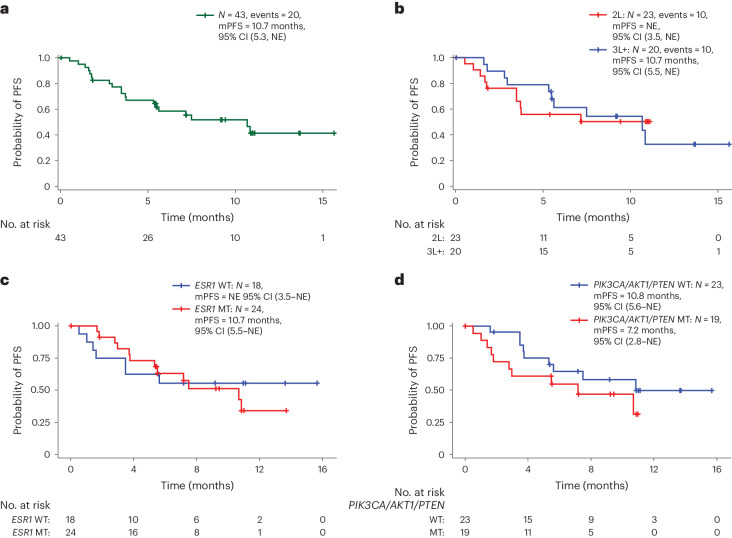
Inhibition of histone lysine acetyltransferases (KATs) KAT6A and KAT6B has shown antitumor activity in estrogen receptor-positive (ER+) breast cancer preclinical models. PF-07248144 is a selective catalytic inhibitor of KAT6A and KAT6B. In the present study, we report the safety, pharmacokinetics (PK), pharmacodynamics, efficacy and biomarker results from the first-in-human, phase 1 dose escalation and dose expansion study (n = 107) of PF-07248144 monotherapy and fulvestrant combination in heavily pretreated ER+ human epidermal growth factor receptor-negative (HER2-) metastatic breast cancer (mBC). The primary objectives of assessing the safety and tolerability and determining the recommended dose for expansion of PF-07248144, as monotherapy and in combination with fulvestrant, were met. Secondary endpoints included characterization of PK and evaluation of antitumor activity, including objective response rate (ORR) and progression-free survival (PFS). Common treatment-related adverse events (any grade; grades 3-4) included dysgeusia (83.2%, 0%), neutropenia (59.8%, 35.5%) and anemia (48.6%, 13.1%). Exposure was approximately dose proportional. Antitumor activity was observed as monotherapy. For the PF-07248144-fulvestrant combination (n = 43), the ORR (95% confidence interval (CI)) was 30.2% (95% CI = 17.2-46.1%) and the median PFS was 10.7 (5.3-not evaluable) months. PF-07248144 demonstrated a tolerable safety profile and durable antitumor activity in heavily pretreated ER+HER2- mBC. These findings establish KAT6A and KAT6B as druggable cancer targets, provide clinical proof of concept and reveal a potential avenue to treat mBC. clinicaltrial.gov registration: NCT04606446 .
© 2024. The Author(s).
Conflict of interest statement
T.M. received honoraria from AstraZeneca, Chugai Pharma, Eisai, Kyowa Kirin, Lilly Japan, Novartis, Pfizer and Taiho Pharmaceutical; had a consulting or advisory role at Eisai and Micin; and received research funding from AstraZeneca, Chugai Pharma, Daiichi Sankyo/AstraZeneca, Eisai, Gilead Sciences, MSD, Novartis, Ono Pharmaceutical, Pfizer, Sanofi and Sysmex. Y.H.P. received honoraria from AstraZeneca, Daiichi Sankyo, Eisai, Lilly, MSD, Novartis, Pfizer and Roche; had a consulting or advisory role at AstraZeneca, Boryung, Daiichi Sankyo, Eisai, Gilead Sciences, Lilly, Menarini, MSD, Novartis, Pfizer and Roche; received research funding from AstraZeneca, Pfizer, Gencurix, Genome Insight, NGeneBio and Roche; and received travel and accommodation expenses from Gilead. D.S. was employed at Texas Oncology; had stock and other ownership interests in Texas Oncology and NEXT Oncology; received honoraria from Syneos Health; had a consulting or advisory role at Guidepoint and Revolution Medicines; and received research funding from Abbvie, ADC Therapeutics, Ascentage Pharma, Biomea Fusion, BioNTech SE, BJ Bioscience, Boehringer Ingelheim, Fate Therapeutics, Gilead Sciences, Immuneering, Kura Oncology, MediLink, Mirati Therapeutics, Monopteros Therapeutics, Navire, NGM Biopharmaceuticals, Nimbus Therapeutics, OncoResponse Inc., Pfizer, Revolution Medicines, Symphoge, Tachyon Therapeutics, Teon Therapeutics and ZielBio. K.Y. received honoraria from AstraZeneca, Chugai Pharma, Daiichi Sankyo/AstraZeneca, Eisai, Fujifilm, Lilly Japan, MSD Oncology, Novartis, Ono Pharmaceutical, Pfizer, Taiho Pharmaceutical and Takeda; had a consulting or advisory role at Chugai Pharma, Eisai, Henlius, Novartis, OncXerna Therapeutics and Ono Pharmaceutical; and received research funding from AstraZeneca/MedImmune, Boehringer Ingelheim, Chugai Pharma, Daiichi Sankyo/AstraZeneca, Eisai, Genmab, Haihe Pharmaceutical, Kyowa Kirin, Lilly, MSD, Nihonkayaku, Novartis, Ono Pharmaceutical, Pfizer, Sanofi, Seagen, Taiho Pharmaceutical and Takeda. E.H. had a consulting or advisory role at AstraZeneca, Daiichi Sankyo, Ellipses Pharma, Genentech/Roche, Greenwich LifeSciences, ITeos Therapeutics, Janssen, Lilly, Loxo, Mersana, Novartis, Olema Pharmaceuticals, Orum Therapeutics, Pfizer, Relay Therapeutics, Seagen, Stemline Therapeutics, Theratechnologies, Tubulis GmbH and Verascity Science; and received research funding from Abbvie, Accutar Biotech, Acerta Pharma, ADC Therapeutics, Akeso Biopharma, Amgen, Aravive, ArQule, Artios, Arvinas, AstraZeneca, AtlasMedx, BeiGene, Black Diamond Therapeutics, Bliss Biopharmaceutical, Boehringer Ingelheim, Cascadian Therapeutics, Clovis Oncology, Compugen, Context Therapeutics, Cullinan Oncology, Curis, CytomX Therapeutics, Daiichi Sankyo, Dana Farber Cancer Hospital, Dantari, Deciphera, Duality Biologics, eFFECTOR Therapeutics, Ellipses Pharma, Elucida Oncology, EMD Serono, Fujifilm, G1 Therapeutics, Genentech/Roche, H3 Biomedicine, Harpoon, Hutchison MediPharma, Immunogen, Immunomedics, Incyte, Infinity Pharmaceuticals, InventisBio, Jacobio, K-Group Beta, Karyopharm Therapeutics, Kind Pharmaceuticals, Leap Therapeutics, Lilly, Loxo, Lycera, MabSpace Biosciences, Macrogenics, MedImmune, Mersana, Merus, Millennium, Molecular Templates, Novartis, Nucana, Olema Pharmaceuticals, OncoMed, Onconova Therapeutics, Oncothyreon, ORIC Pharmaceuticals, Orinove, Orum Therapeutics, Pfizer, PharmaMar, Pieris Pharmaceuticals, Pionyr, Plexxikon, Prelude Therapeutics, ProfoundBio, Radius Health, Regeneron, Relay Therapeutics, Repertoire Immune Medicines, Rgenix, Seagen, Sermonix Pharmaceuticals, Shattuck Labs, Stem CentRx, Sutro Biopharma, Syndax, Syros Pharmaceuticals, Taiho Pharmaceutical, TapImmune Inc, Tesaro, Tolmar, Torque, Treadwell Therapeutics, Verastem, Zenith Epigenetics and Zymeworks. S.-B.K. holds stock and other ownership Interests of Genopeaks; received honoraria from DAEHWA Pharmaceutical, Kalbe Farma and LegoChem Biosciences; had a consulting or advisory role at AstraZeneca, BeiGene, DAEHWA Pharmaceutical, Daiichi Sankyo/AstraZeneca, Ensol Biosciences, ISU Abxis, Lilly and OBI Pharma; and received research funding from Genzyme. J.H.K. received honoraria from Roche Korea, AstraZeneca Korea, Lilly Korea, Roche diagnostics and Roche; had a consulting or advisory role at Bixink, Eisai Korea, Roche, MSD Korea, Everest Medicine and Yuhan; and received research funding from Ono Pharma Korea, Roche and Eisai. H.I. received honoraria from AstraZeneca, Chugai, Daiichi Sankyo, Kyowa Kirin, Lilly, MSD, Pfizer and Taiho; had a consulting or advisory role at AstraZeneca, Chugai, Daichi Sankyo, Gilead, Lilly, MSD and Pfizer; and received research funding from AstraZeneca, Chugai and Daiichi Sankyo. T.Y. received honoraria from AstraZeneca, Chugai Pharma, Daiichi Sankyo, Eisai, Kyowa Kirin, Lilly, Pfizer and Taiho Pharmaceutical; and received research funding from AstraZeneca, Chugai Pharma, Daiichi Sankyo, Kyowa Kirin, Lilly, MSD, Nihonkayaku, Pfizer, Seagen and Taiho Pharmaceutical. R.M.L. received honoraria from Pfizer; had a consulting or advisory role at Eli Lilly, Novartis, Pfizer, Celcuity, Gilead Sciences and Biotheryx; and received research funding to institution from Eli Lilly, Novartis, Pfizer, Puma, Zentalis, Celcuity, Arvinas and Accutar Biotechnology. T.D.C. received honoraria from Lilly, Specialised Therapeutics, Roche, MSD and The Limbic; had a consulting or advisory role for AstraZeneca/MedImmune, Merck KGaA, Takeda, Merck/Pfizer, Ipsen, AstraZeneca, Daiichi Sankyo, Janssen and Roche; was a member of Speakers’ Bureau of AstraZeneca/MedImmune; and received research funding from Abbvie, Amgen, Bayer, BeiGene, Clovis Oncology, Daiichi Sankyo/AstraZeneca, Exelixis, Immutep, Janssen Oncology, MSD Oncology, Pfizer, BridgeBio Pharma and Bristol Myers Squibb GmbH & Co. K.G. held stock and other ownership Interests of ClinicIQ; and received travel and accommodation expenses from AstraZeneca, Daiichi Sankyo/UCB Japan and Boehringer Ingelheim. F.Y. received honoraria from Daiichi Sankyo, Merck, AstraZeneca, Grail, Gilead, Stemline, Eli Lilly, SeaGen and GE; and received research funding from Pfizer, Gilead, Merck, Agendia and Genentech. S.-A.I. received honoraria from MSD Korea; had a consulting or advisory role at AstraZeneca, Bertis, Daiichi Sankyo, Eisai, Gilead, Lilly, MSD, Novartis, Pfizer and Roche; and received research funding from AstraZeneca, Daiichi Sankyo, Boryung Pharm, Daewoong Pharm, Eisai, Roche and Pfizer. G.J.L. received honoraria from Pfizer; had a consulting or advisory role at Pfizer and AbbVie; and received research funding from AbbVie, Amgen, Genentech and Pfizer (all study support to Institution for investigator-initiated studies) and Cooperative Research Centre for Cancer Therapeutic, Australia (laboratory funding). H.S.R. had a consulting or advisory role at Daiichi Sankyo, Eisai, Mylan, Napo Pharmaceuticals and Puma Biotechnology; and received research funding from Astellas Pharma, AstraZeneca, Daiichi Sankyo, Genentech/Roche, Gilead Sciences, GSK, Lilly, Merck, Novartis, OBI Pharma, Pfizer, Stemline Therapeutics, Taiho Oncology and Veru. P.M.L.R. received honoraria from Five Prime Therapeutics; had a consulting or advisory role at Abbvie, ABL Bio, Actuate Therapeutics, Agenus, Amgen, AstraZeneca, Atreca, BAKX Therapeutics, Boehringer Ingelheim, Compass Therapeutics, Cullinan Oncology, DAAN Biotherapeutics, EMD Serono, GSK, I-Mab, ImCheck therapeutics, IQvia, Kineta, Kyowa Kirin International, Mekanistic Therapeutics, Mersana, Molecular Templates, Neurotrials Research, Pfizer, QED Therapeutics, Qualigen Therapeutics, Quanta Therapeutics, Relay Therapeutics, Roche/Genentech, Roivant, Scenic Biotech, Schrodinger, Seagen, Sotio, ST Cube, Stemline Therapeutics, Takeda and Zentalis; received research funding from Genentech; and received travel and accommodation expenses from Genentech. M.L. has a patent royalty from the Johns Hopkins University; is employed at Pfizer; and owns stock and other ownership interests of Pfizer. M.L., C.L.C., A.S., L.L. and M.S. are employed at Pfizer; and own stock and other ownership interests of Pfizer. The other authors have no competing interests.
Figures








References
-
- San-Miguel, J. F. et al. Panobinostat plus bortezomib and dexamethasone versus placebo plus bortezomib and dexamethasone in patients with relapsed or relapsed and refractory multiple myeloma: a multicentre, randomised, double-blind phase 3 trial. Lancet Oncol.15, 1195–1206 (2014). 10.1016/S1470-2045(14)70440-1 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
