

Guillain-Barré Syndrome in a Patient Receiving Anti-Tumor Necrosis Factor for Crohn Disease: Coincidence or Consequence?
- PMID: 38824385
- PMCID: PMC11155199
- DOI: 10.12659/AJCR.943709
Guillain-Barré Syndrome in a Patient Receiving Anti-Tumor Necrosis Factor for Crohn Disease: Coincidence or Consequence?
Abstract
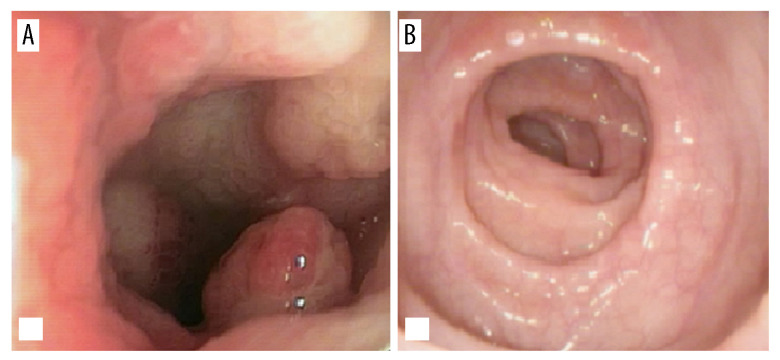
BACKGROUND Antibodies against tumor necrosis factor alpha (anti-TNF-alpha) are currently widely used in the treatment of inflammatory bowel diseases (IBD), despite a number of reported adverse effects. Diverse neurologic syndromes, including the Guillain-Barre syndrome (GBS), an immune-mediated disease characterized by evolving ascending limb weakness, sensory loss, and areflexia, have been described in association with anti-TNF-alpha therapy. CASE REPORT A 45-year-old White woman was in follow-up with fistulizing ileocolonic Crohn disease using combination therapy (infliximab plus azathioprine) as CD maintenance therapy. After 3 years of this immunosuppressive therapy, she presented with symmetrical and ascending paresis in the lower limbs, and later in the upper limbs, in addition to reduced reflexes in the knees, 1 day after an infliximab infusion. The patient was hospitalized and treatment for CD was suspended. Neurophysiology studies demonstrated a pattern compatible with acute inflammatory demyelinating polyradiculopathy, with predominantly motor involvement, consistent with Guillain-Barre syndrome (GBS). Clinical, laboratory, and imaging exams were unremarkable. She was treated with intravenous immunoglobulins, with a progressive and complete resolution of neurological symptoms. After 1-year follow-up, she presented with active Crohn disease, and we opted for treating her with vedolizumab, with which she achieved clinical and endoscopic remission. CONCLUSIONS Patients receiving biological therapy with anti-TNF-alpha agents should be monitored for central or peripheral neurological signs and symptoms. The development of GBS can be secondary to anti-TNF-alpha treatment. The positive temporal relationship with TNF-alpha therapy and onset of neurological symptoms reinforces this possibility.
Conflict of interest statement
Figures
Similar articles
-
Guillain-Barré syndrome in association with antitumour necrosis factor therapy: a case of mistaken identity.BMJ Case Rep. 2017 Jul 5;2017:bcr2017219481. doi: 10.1136/bcr-2017-219481. BMJ Case Rep. 2017. PMID: 28679512 Free PMC article.
-
Guillain-Barré syndrome during adalimumab therapy for Crohn´s disease: coincidence or consequence?Scand J Gastroenterol. 2017 Apr;52(4):473-476. doi: 10.1080/00365521.2016.1263682. Epub 2016 Dec 8. Scand J Gastroenterol. 2017. PMID: 27931132
-
Severe Guillain-Barré syndrome in a patient receiving anti-TNF therapy. Consequence or coincidence. A case-based review.Clin Rheumatol. 2013 Sep;32(9):1407-12. doi: 10.1007/s10067-013-2272-9. Epub 2013 May 11. Clin Rheumatol. 2013. PMID: 23666317 Review.
-
Guillain-Barre in a patient with ankylosing spondylitis secondary to ulcerative colitis on infliximab therapy.Clin Rheumatol. 2009 Jun;28 Suppl 1:S53-5. doi: 10.1007/s10067-009-1154-7. Epub 2009 Mar 11. Clin Rheumatol. 2009. PMID: 19277812
-
Is secukinumab a safe alternative treatment for ankylosing spondylitis with Guillain Barré syndrome after anti-TNF-α treatment? Case report and literature review.Clin Rheumatol. 2017 May;36(5):1197-1199. doi: 10.1007/s10067-017-3573-1. Epub 2017 Feb 23. Clin Rheumatol. 2017. PMID: 28233109 Review.
References
-
- Cohen LB, Nanau RM, Delzor F, Neuman MG. Biologic therapies in inflammatory bowel disease. Transl Res. 2014;163(6):533–56. - PubMed
-
- Sehgal P, Colombel JF, Narula N. Adverse events during anti-TNFα therapies in IBD (Excluding Infections and Malignancies): When to stop, continue, or switch therapies. Inflamm Bowel Dis. 2016;22(5):1239–45. - PubMed
-
- Sousa P, Allez M. Complications of biologics in inflammatory bowel disease. Curr Opin Gastroenterol. 2015;31(4):296–302. - PubMed
-
- Marchetti F, Roveran M, Currò F, et al. Guillain-Barré syndrome. Med e Bambino. 2020;39(3):179–82.
-
- Shahrizaila N, Lehmann HC, Kuwabara S. Guillain-Barré syndrome. Lancet. 2021;397(10280):1214–28. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
