

Epicardial placement of human placental membrane allografts in coronary artery bypass graft surgery is associated with reduced postoperative atrial fibrillation: a pilot study for a future multi-center randomized controlled trial
- PMID: 38824517
- PMCID: PMC11143688
- DOI: 10.1186/s13019-024-02822-8
Epicardial placement of human placental membrane allografts in coronary artery bypass graft surgery is associated with reduced postoperative atrial fibrillation: a pilot study for a future multi-center randomized controlled trial
Erratum in
-
Correction: Epicardial placement of human placental membrane allografts in coronary artery bypass graft surgery is associated with reduced postoperative atrial fibrillation: a pilot study for a future multi-center randomized controlled trial.J Cardiothorac Surg. 2024 Jul 1;19(1):410. doi: 10.1186/s13019-024-02942-1. J Cardiothorac Surg. 2024. PMID: 38951830 Free PMC article. No abstract available.
Abstract
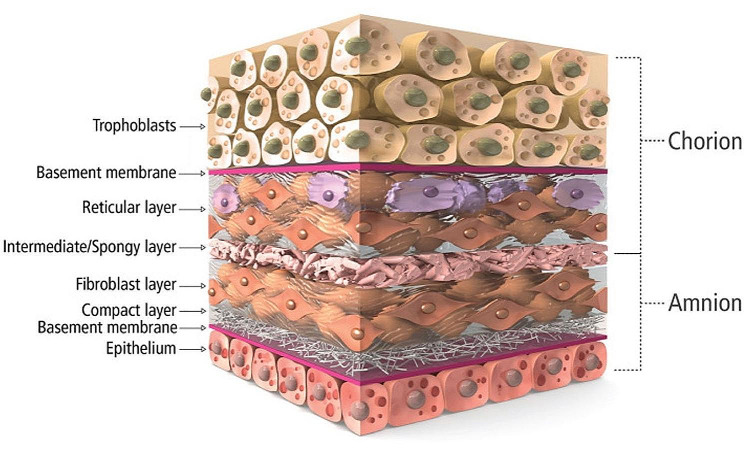
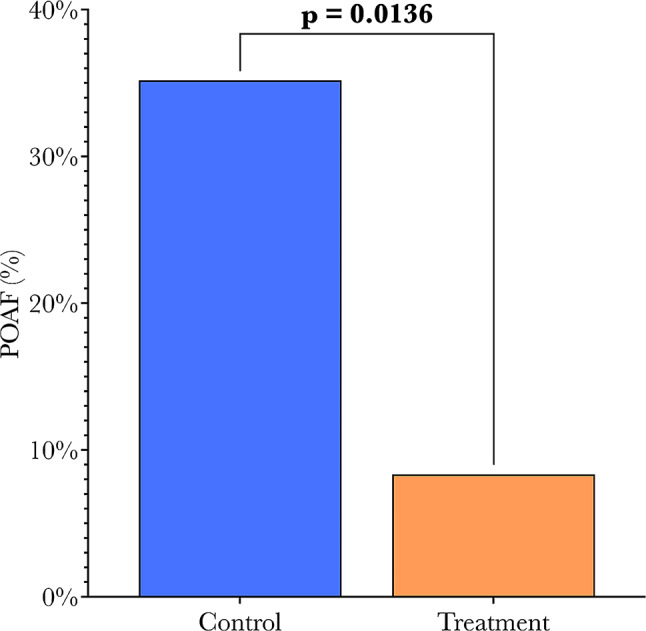
Background: Post-operative atrial fibrillation (POAF) occurs in up to 40% of patients following coronary artery bypass grafting (CABG) and is associated with a higher risk of stroke and mortality. This study investigates how POAF may be mitigated by epicardial placement of aseptically processed human placental membrane allografts (HPMAs) before pericardial closure in CABG surgery. This study was conducted as a pilot feasibility study to collect preliminary for a forthcoming multi-center randomized controlled trial.
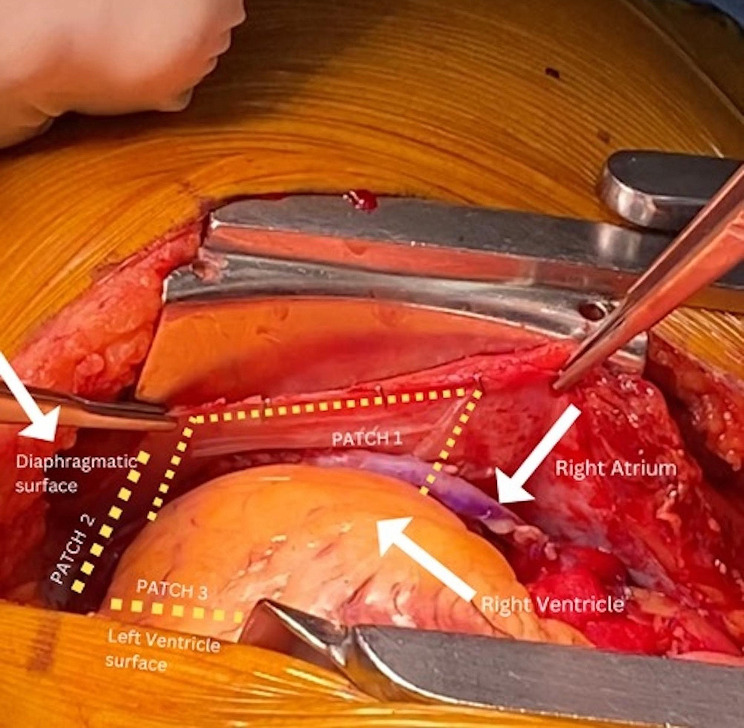
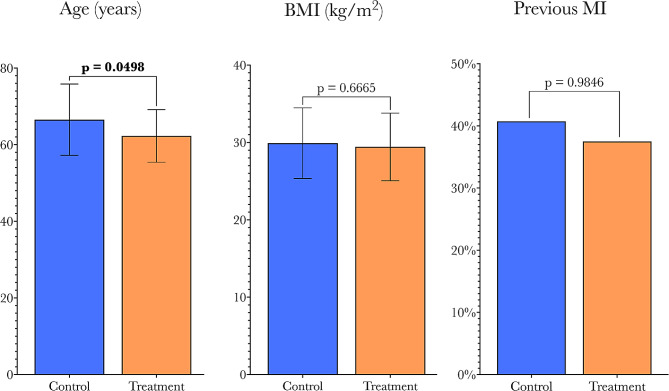
Methods: This retrospective observational study of patients undergoing CABG surgery excluded patients with pre-operative heart failure, chronic kidney disease, or a history of atrial fibrillation. The "treatment" group (n = 24) had three HPMAs placed epicardially following cardiopulmonary bypass decannulation but before partial pericardial approximation and chest closure. The only difference in clinical protocol for the control group (n = 54) was that they did not receive HPMA.
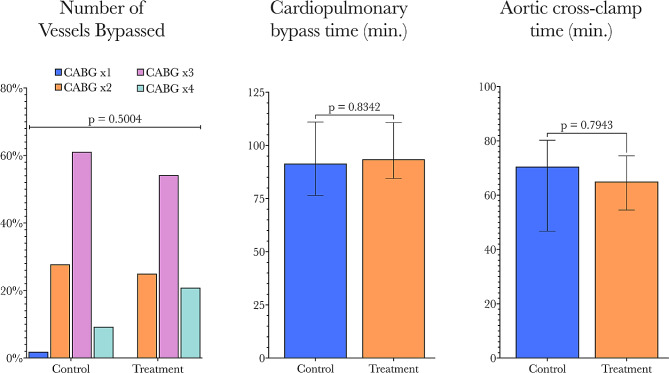
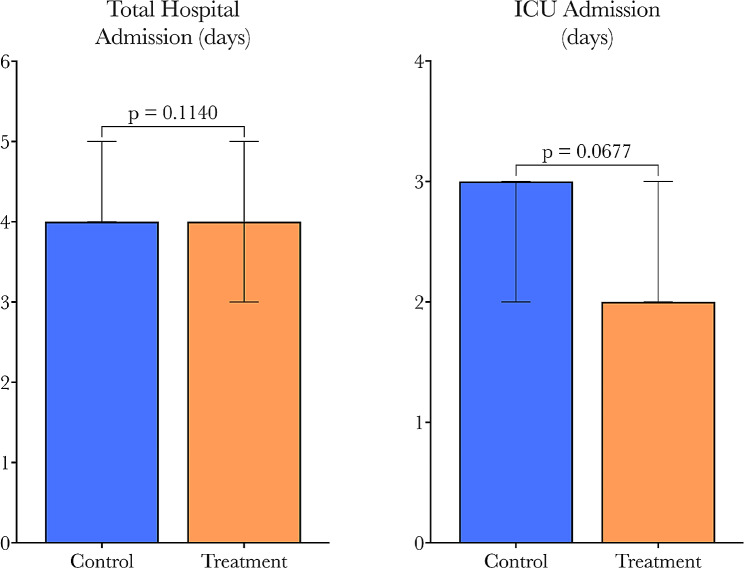
Results: HPMA-treated patients saw a significant, greater than four-fold reduction in POAF incidence compared to controls (35.2-8.3%, p = 0.0136). Univariate analysis demonstrated that HPMA treatment was associated with an 83% reduction in POAF (OR = 0.17, p = 0.0248). Multivariable analysis yielded similar results (OR = 0.07, p = 0.0156) after controlling for other covariates. Overall length of stay (LOS) between groups was similar, but ICU LOS trended lower with HPMA treatment (p = 0.0677). Post-operative inotrope and vasopressor requirements were similar among groups. There was no new-onset post-operative heart failure, stroke, or death reported up to thirty days in either group.
Conclusions: Epicardial HPMA placement can be a simple intervention at the end of CABG surgery that may provide a new approach to reduce post-operative atrial fibrillation by modulating local inflammation, possibly reducing ICU and hospital stay, and ultimately improving patient outcomes.
Keywords: Aseptically processed human placental membrane allograft.; Coronary artery bypass grafting; Post-operative atrial fibrillation.
© 2024. The Author(s).
Conflict of interest statement
ZK serves as a consultant for MTF Biologics. PH, EC, and ML are employed by MTF Biologics. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be a potential conflict of interest.
Figures
Similar articles
-
A retrospective study on atrial fibrillation after coronary artery bypass grafting surgery at The National Heart Institute, Kuala Lumpur.F1000Res. 2018 Feb 8;7:164. doi: 10.12688/f1000research.13244.2. eCollection 2018. F1000Res. 2018. PMID: 30254739 Free PMC article.
-
Posterior pericardiotomy and the prevention of post-operative atrial fibrillation and cardiac tamponade in isolated coronary artery bypass grafting - A retrospective analysis.J Cardiothorac Surg. 2024 Apr 24;19(1):263. doi: 10.1186/s13019-024-02569-2. J Cardiothorac Surg. 2024. PMID: 38659034 Free PMC article.
-
[Predictors of New-Onset Atrial Fibrillation in Patients With Chronic Coronary Artery Disease After Coronary Artery Bypass Grafting: a Prospective, Observational, Single-Centre, Non-Randomized Study].Kardiologiia. 2024 Oct 31;64(10):40-47. doi: 10.18087/cardio.2024.10.n2511. Kardiologiia. 2024. PMID: 39526517 Russian.
-
Posterior pericardiotomy to prevent new-onset atrial fibrillation after coronary artery bypass grafting: a systematic review and meta-analysis of 10 randomized controlled trials.J Cardiothorac Surg. 2021 Aug 14;16(1):233. doi: 10.1186/s13019-021-01611-x. J Cardiothorac Surg. 2021. PMID: 34391454 Free PMC article.
-
Potential use of statins to prevent atrial fibrillation after coronary artery bypass surgery.Ann Pharmacother. 2008 Feb;42(2):253-8. doi: 10.1345/aph.1K590. Epub 2008 Jan 15. Ann Pharmacother. 2008. PMID: 18198239 Review.
Cited by
-
Correction: Epicardial placement of human placental membrane allografts in coronary artery bypass graft surgery is associated with reduced postoperative atrial fibrillation: a pilot study for a future multi-center randomized controlled trial.J Cardiothorac Surg. 2024 Jul 1;19(1):410. doi: 10.1186/s13019-024-02942-1. J Cardiothorac Surg. 2024. PMID: 38951830 Free PMC article. No abstract available.
-
Surgical Methods and Devices for Atrial Fibrillation.Rev Cardiovasc Med. 2025 Apr 23;26(4):26841. doi: 10.31083/RCM26841. eCollection 2025 Apr. Rev Cardiovasc Med. 2025. PMID: 40351669 Free PMC article. Review.
References
-
- Heron M, Deaths. Leading Causes for 2018 [Internet]. National Center for Health Statistics; 2021 May [cited 2024 Feb 29]. https://stacks.cdc.gov/view/cdc/104186.
-
- Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in partnership with the European Society of Cardiology and in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. J Am Coll Cardiol. 2011;57(11):e101–98. doi: 10.1016/j.jacc.2010.09.013. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
