

Stem anteversion is not affected by proximal femur geometry in robotic-assisted total hip arthroplasty
- PMID: 38824601
- PMCID: PMC11144328
- DOI: 10.1186/s42836-024-00248-0
Stem anteversion is not affected by proximal femur geometry in robotic-assisted total hip arthroplasty
Abstract
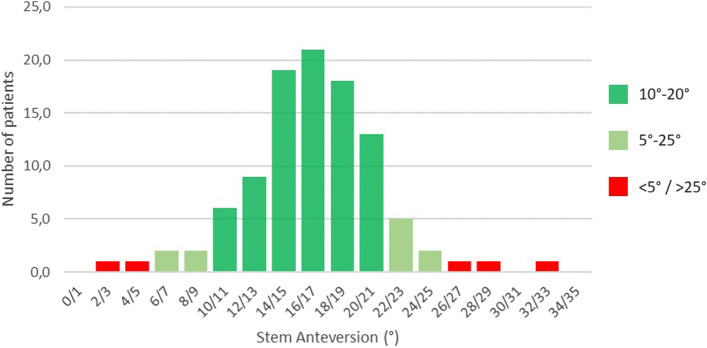
Background: In the present study, the surgeon aimed to align the stem at 5° to 25° in anteversion. The robotic technology was used to measure stem anteversion with respect to proximal femur anteversion at different levels down the femur.
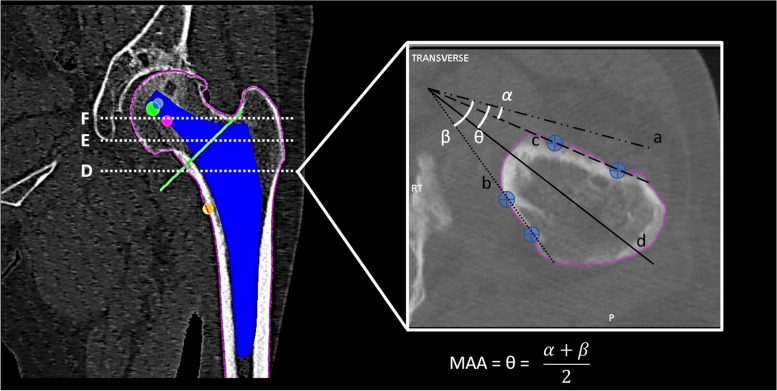
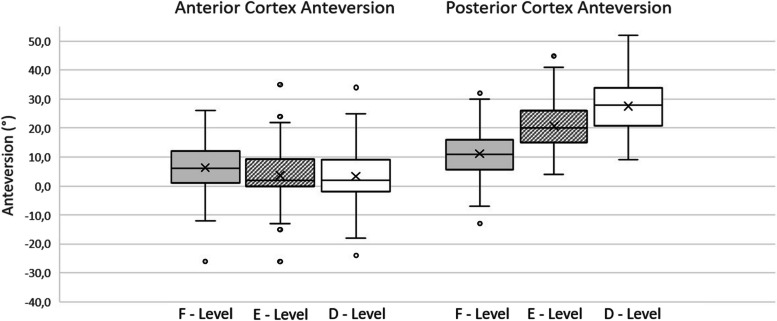
Methods: A total of 102 consecutive patients underwent robotic-arm-assisted total hip arthroplasty (RTHA). 3D CT-based preoperative planning was performed to determine femoral neck version (FNV), posterior cortex anteversion (PCA), anterior cortex anteversion (ACA), and femoral metaphyseal axis anteversion (MAA) at 3 different levels: D (10 mm above lesser trochanter), E (the midpoint of the planned neck resection line) and F (head-neck junction). The robotic system was used to define and measure stem anteversion during surgery.
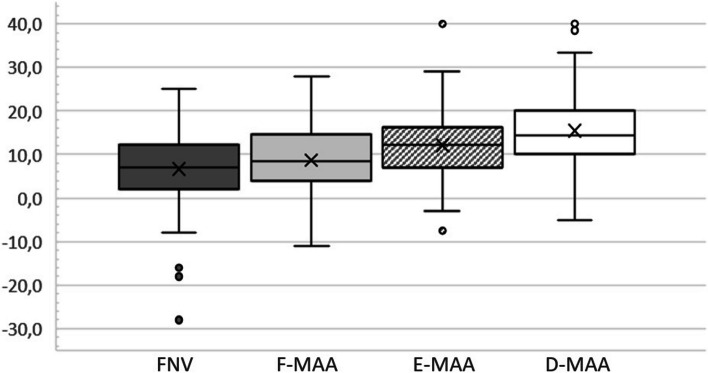
Results: Mean FNV was 6.6° (SD: 8.8°) and the mean MAA was consistently significantly higher than FNV, growing progressively from proximal to distal. Mean SV was 16.4° (SD: 4.7°). There was no statistically significant difference (P = 0.16) between SV and MAA at the most distal measured level. In 96.1% cases, the stem was positioned inside the 5°-25° anteversion range.
Conclusions: Femoral anteversion progressively increased from neck to proximal metaphysis. Aligning the stem close to femoral anteversion 10 mm above the lesser trochanter often led to the desired component anteversion.
Keywords: Combined anteversion; Robotic arm-assisted surgery; Stem anteversion; Total hip arthroplasty.
© 2024. The Author(s).
Conflict of interest statement
F.C. reports a relationship with Stryker Orthopaedics that includes: consulting or advisory and travel reimbursement. Royalties from Stryker Orthopaedics; M.P. reports a relationship with AB Medica s.p.a. that includes: employment; F.Z.: Guest Editor for
Figures
References
LinkOut - more resources
Full Text Sources