

The relationship between low levels of albuminuria and mortality among adults without major cardiovascular risk factors
- PMID: 38825979
- PMCID: PMC11629963
- DOI: 10.1093/eurjpc/zwae189
The relationship between low levels of albuminuria and mortality among adults without major cardiovascular risk factors
Abstract
Aims: The aim of this study is to determine whether elevated levels of albuminuria within the low range [urinary albumin-to-creatinine ratio (UACR) <30 mg/g] are linked to cardiovascular death in adults lacking major cardiovascular risk factors.
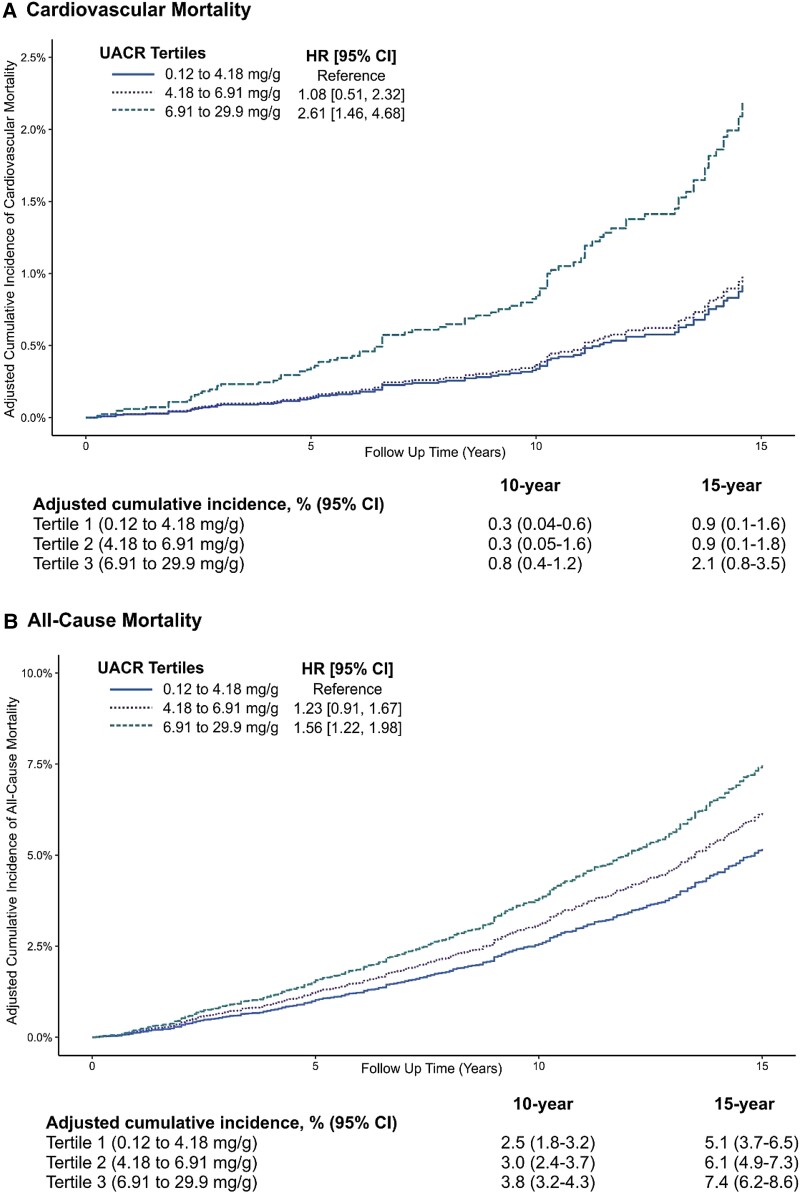
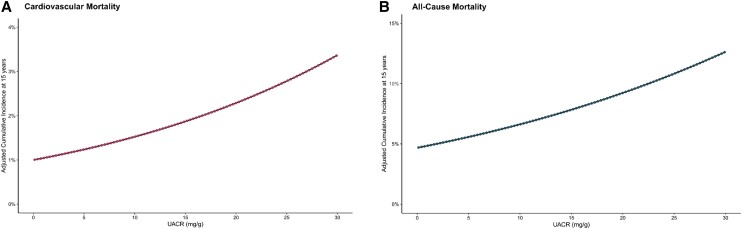
Methods and results: The association between UACR and cardiovascular mortality was investigated among 12 835 participants in the 1999-2014 National Health and Nutrition Examination Survey using Cox proportional hazard models and confounder-adjusted survival curves. We excluded participants with baseline cardiovascular disease, hypertension, diabetes, pre-diabetes, an estimated glomerular filtration rate <60 mL/min/1.73 m2, currently pregnant, and those who received dialysis last year. Over a median follow-up of 12.3 years, 110 and 621 participants experienced cardiovascular and all-cause mortality. In multivariable-adjusted models, each doubling of UACR was associated with a 36% higher risk of cardiovascular death [hazard ratio (HR) 1.36, 95% confidence interval (CI) 1.02-1.82] and a 24% higher risk of all-cause mortality (HR 1.24, 95% CI 1.10-1.39). The 15-year adjusted cumulative incidences of cardiovascular mortality were 0.91, 0.99, and 2.1% for UACR levels of <4.18, 4.18 to <6.91, and ≥6.91 mg/g, respectively. The 15-year adjusted cumulative incidences of all-cause mortality were 5.1, 6.1, and 7.4% for UACR levels of <4.18, 4.18 to <6.91, and ≥6.91 mg/g, respectively.
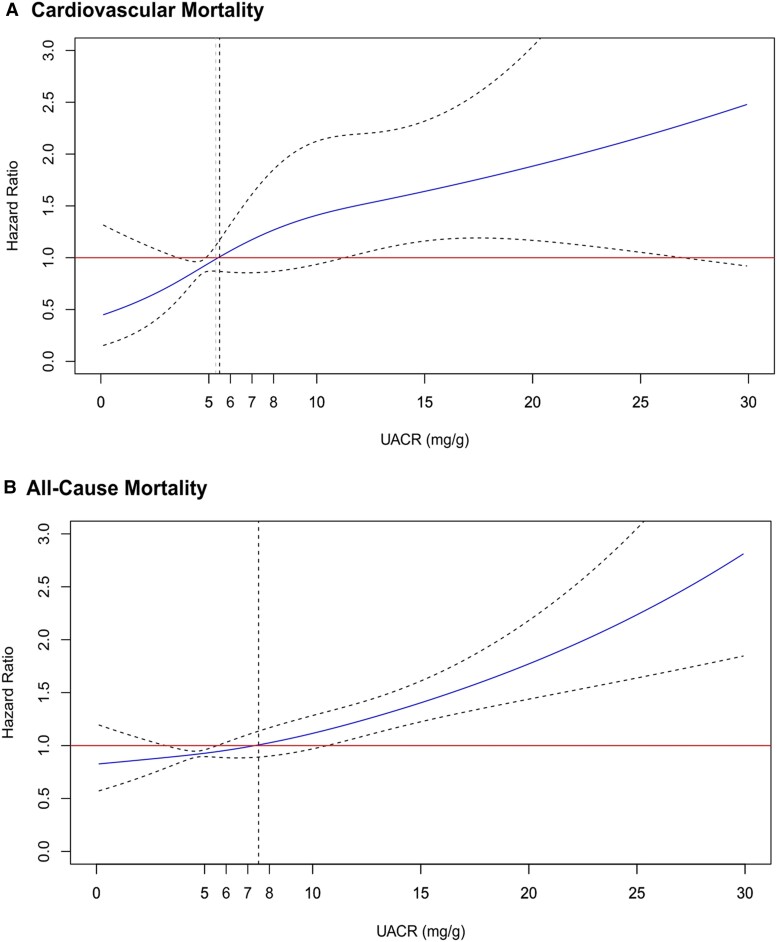
Conclusion: Adults with elevated levels of albuminuria within the low range (UACR <30 mg/g) and no major cardiovascular risk factors had elevated risks of cardiovascular and all-cause mortality. The risk increased linearly with higher albuminuria levels. This emphasizes a risk gradient across all albuminuria levels, even within the supposedly normal range, adding to the existing evidence.
Keywords: Albuminuria; All-cause mortality; Cardiovascular mortality; Low-grade albuminuria; NHANES; UACR.
Plain language summary
In this study of 12 835 adults without major cardiovascular risk factors (such as hypertension, cardiovascular disease, diabetes, pre-diabetes, or chronic kidney disease), we investigated the association between higher albuminuria levels within the low range [urine albumin-to-creatinine ratio (UACR) <30 mg/g] and both cardiovascular and all-cause mortality. Our findings revealed a linear increase in excess risk for both outcomes with rising albuminuria among relatively healthy adults. Each doubling of albuminuria was associated with a 36% higher risk of cardiovascular death [hazard ratio (HR) 1.36, 95% confidence interval (CI) 1.02–1.82] and a 24% higher risk of all-cause mortality (HR 1.24, 95% CI 1.10–1.39). Each 10 mg/g increase in albuminuria was associated with a 66% higher risk of cardiovascular mortality (HR 1.66, 95% CI 1.20–2.28) and a 41% higher risk of all-cause mortality (HR 1.41, 95% CI 1.17–1.68). These results challenge the assumption that UACR values below 30 mg/g are non-prognostic in adults without major cardiovascular risk factors.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Conflict of interest statement
Conflict of interest: none declared.
Figures
Update of
-
The relationship between low levels of albuminuria and cardiovascular mortality among apparently healthy adults.medRxiv [Preprint]. 2023 Dec 24:2023.12.21.23300378. doi: 10.1101/2023.12.21.23300378. medRxiv. 2023. Update in: Eur J Prev Cardiol. 2024 Dec 4;31(17):2046-2055. doi: 10.1093/eurjpc/zwae189. PMID: 38196576 Free PMC article. Updated. Preprint.
Comment in
-
Do low levels of albuminuria predict mortality among young adults without major cardiovascular risk factors?Eur J Prev Cardiol. 2024 Dec 4;31(17):2056-2057. doi: 10.1093/eurjpc/zwae223. Eur J Prev Cardiol. 2024. PMID: 38970505 No abstract available.
References
-
- Rose B. Pathophysiology of Renal Disease. 2nd ed. New York: McGraw Hill; 1987.
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Guideline Development Work Group . KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 2013;3:136–150.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
