

Interpretable machine learning model for early prediction of delirium in elderly patients following intensive care unit admission: a derivation and validation study
- PMID: 38828233
- PMCID: PMC11140063
- DOI: 10.3389/fmed.2024.1399848
Interpretable machine learning model for early prediction of delirium in elderly patients following intensive care unit admission: a derivation and validation study
Abstract
Background and objective: Delirium is the most common neuropsychological complication among older adults admitted to the intensive care unit (ICU) and is often associated with a poor prognosis. This study aimed to construct and validate an interpretable machine learning (ML) for early delirium prediction in older ICU patients.
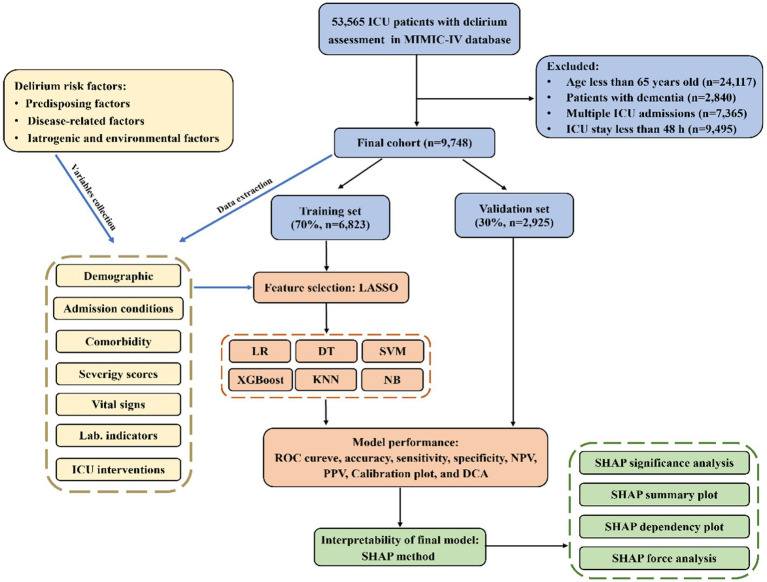
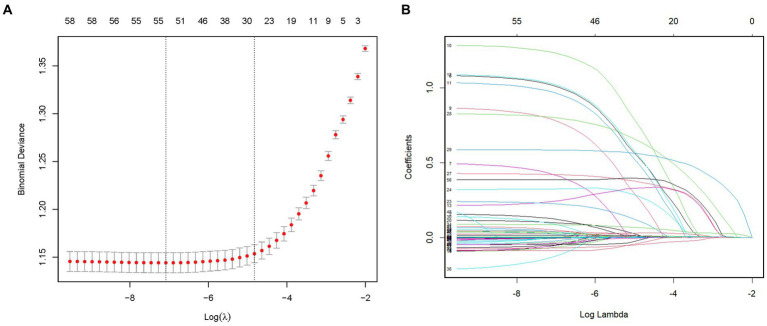
Methods: This was a retrospective observational cohort study and patient data were extracted from the Medical Information Mart for Intensive Care-IV database. Feature variables associated with delirium, including predisposing factors, disease-related factors, and iatrogenic and environmental factors, were selected using least absolute shrinkage and selection operator regression, and prediction models were built using logistic regression, decision trees, support vector machines, extreme gradient boosting (XGBoost), k-nearest neighbors and naive Bayes methods. Multiple metrics were used for evaluation of performance of the models, including the area under the receiver operating characteristic curve (AUC), accuracy, sensitivity, specificity, recall, F1 score, calibration plot, and decision curve analysis. SHapley Additive exPlanations (SHAP) were used to improve the interpretability of the final model.
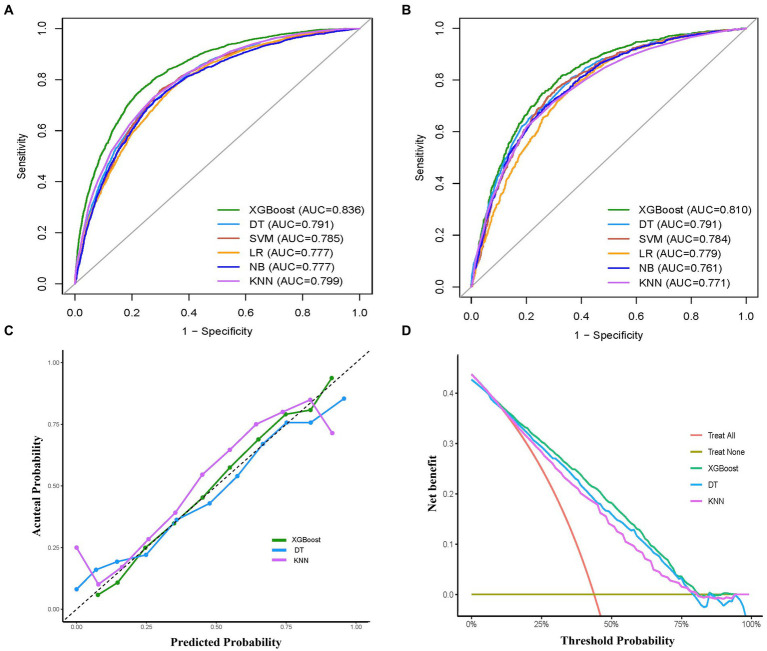
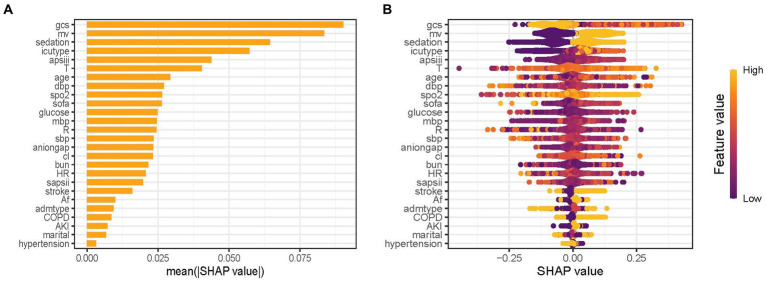
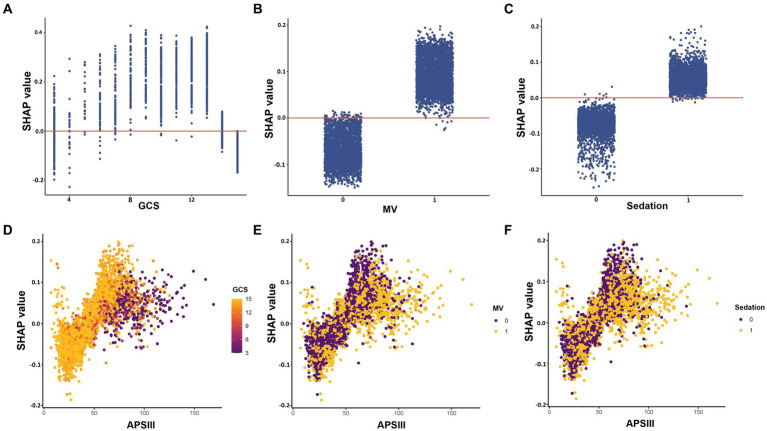
Results: Nine thousand seven hundred forty-eight adults aged 65 years or older were included for analysis. Twenty-six features were selected to construct ML prediction models. Among the models compared, the XGBoost model demonstrated the best performance including the highest AUC (0.836), accuracy (0.765), sensitivity (0.713), recall (0.713), and F1 score (0.725) in the training set. It also exhibited excellent discrimination with AUC of 0.810, good calibration, and had the highest net benefit in the validation cohort. The SHAP summary analysis showed that Glasgow Coma Scale, mechanical ventilation, and sedation were the top three risk features for outcome prediction. The SHAP dependency plot and SHAP force analysis interpreted the model at both the factor level and individual level, respectively.
Conclusion: ML is a reliable tool for predicting the risk of critical delirium in elderly patients. By combining XGBoost and SHAP, it can provide clear explanations for personalized risk prediction and more intuitive understanding of the effect of key features in the model. The establishment of such a model would facilitate the early risk assessment and prompt intervention for delirium.
Keywords: ICU; delirium; elderly; explainable machine learning; prediction model.
Copyright © 2024 Tang, Ma and Xu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Construction and validation of prognostic models in critically Ill patients with sepsis-associated acute kidney injury: interpretable machine learning approach.J Transl Med. 2023 Jun 22;21(1):406. doi: 10.1186/s12967-023-04205-4. J Transl Med. 2023. PMID: 37349774 Free PMC article.
-
Interpretable machine learning model for early prediction of 28-day mortality in ICU patients with sepsis-induced coagulopathy: development and validation.Eur J Med Res. 2024 Jan 3;29(1):14. doi: 10.1186/s40001-023-01593-7. Eur J Med Res. 2024. PMID: 38172962 Free PMC article.
-
Clinical decision support systems for 3-month mortality in elderly patients admitted to ICU with ischemic stroke using interpretable machine learning.Digit Health. 2024 Sep 17;10:20552076241280126. doi: 10.1177/20552076241280126. eCollection 2024 Jan-Dec. Digit Health. 2024. PMID: 39314817 Free PMC article.
-
Interpretable machine learning model to predict surgical difficulty in laparoscopic resection for rectal cancer.Front Oncol. 2024 Feb 6;14:1337219. doi: 10.3389/fonc.2024.1337219. eCollection 2024. Front Oncol. 2024. PMID: 38380369 Free PMC article. Review.
-
Methodological Review of Classification Trees for Risk Stratification: An Application Example in the Obesity Paradox.Nutrients. 2025 May 31;17(11):1903. doi: 10.3390/nu17111903. Nutrients. 2025. PMID: 40507172 Free PMC article. Review.
Cited by
-
Enhanced machine learning predictive modeling for delirium in elderly ICU patients with COPD and respiratory failure: A retrospective study based on MIMIC-IV.PLoS One. 2025 Mar 20;20(3):e0319297. doi: 10.1371/journal.pone.0319297. eCollection 2025. PLoS One. 2025. PMID: 40112262 Free PMC article.
-
Machine learning prediction model with shap interpretation for chronic bronchitis risk assessment based on heavy metal exposure: a nationally representative study.BMC Pulm Med. 2025 May 22;25(1):252. doi: 10.1186/s12890-025-03724-8. BMC Pulm Med. 2025. PMID: 40405146 Free PMC article.
-
Predicting ICU Delirium in Critically Ill COVID-19 Patients Using Demographic, Clinical, and Laboratory Admission Data: A Machine Learning Approach.Life (Basel). 2025 Jun 30;15(7):1045. doi: 10.3390/life15071045. Life (Basel). 2025. PMID: 40724546 Free PMC article.
-
Development of a risk prediction model for sepsis-related delirium based on multiple machine learning approaches and an online calculator.PLoS One. 2025 Jul 16;20(7):e0323831. doi: 10.1371/journal.pone.0323831. eCollection 2025. PLoS One. 2025. PMID: 40668815 Free PMC article.
-
Development and internal verification of nomogram for forecasting delirium in the elderly admitted to intensive care units: an analysis of MIMIC-IV database.Front Neurol. 2025 May 13;16:1580125. doi: 10.3389/fneur.2025.1580125. eCollection 2025. Front Neurol. 2025. PMID: 40433619 Free PMC article.
References
LinkOut - more resources
Full Text Sources