

Evaluafion of the efficacy of wall shear stress in carotid artery stenting
- PMID: 38828314
- PMCID: PMC11140617
- DOI: 10.1016/j.heliyon.2024.e31383
Evaluafion of the efficacy of wall shear stress in carotid artery stenting
Abstract
Objective: To characterize the value of carotid wall shear stress (WSS) following carotid artery stenting (CAS) in patients with carotid stenosis.
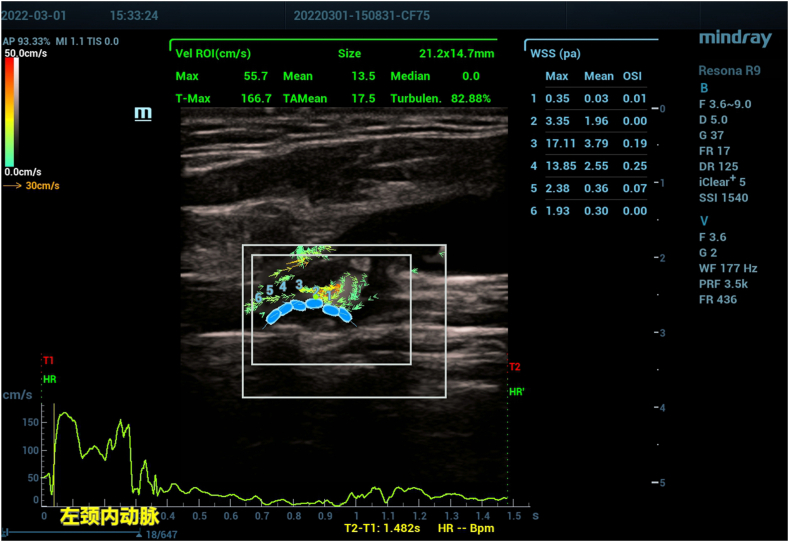
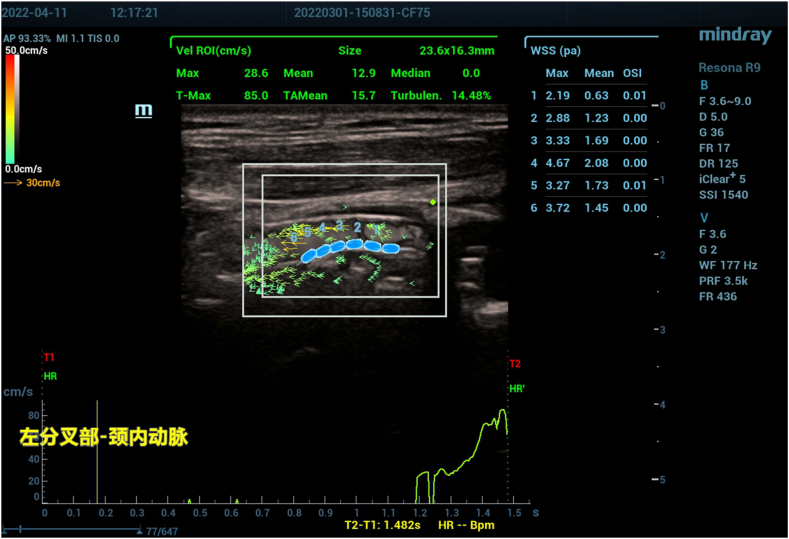
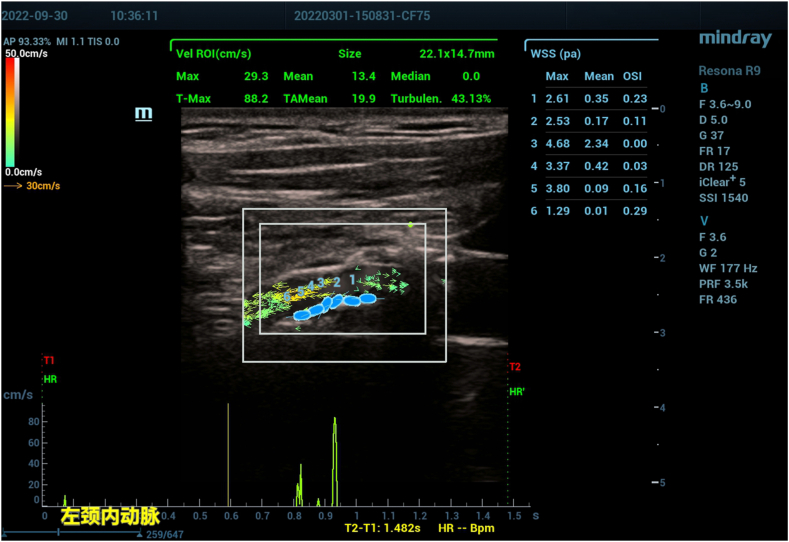
Methods: Twenty-eight patients with carotid stenosis treated with CAS between March 2021 to May 2022 in the eighth medical center of the PLA General Hospital were selected for our study. Carotid ultrasound was performed before the operation, one week post-operation, and six months post-operation. Carotid artery WSS was detected by blood flow vector imaging, and the changes in WSS before and after the operation were collected. Genetic testing of drugs was detected for patients with restenosis.
Results: Pre-operative WSS of the proximal, narrowest region, and distal carotid arteries in patients with ischemic carotid artery stenosis was 7.88 ± 3.18Pa, 14.36 ± 6.66Pa, and 1.55 ± 1.15Pa, respectively. Comparatively, pre-operative WSS of the proximal, narrowest region and distal carotid arteries in patients without ischemic symptoms was 5.02 ± 1.99Pa, 9.68 ± 4.23Pa, and 1.10 ± 0.68Pa, respectively, with a significant difference between the two groups (p < 0.001). Overall WSS of the proximal, narrowest region, and distal carotid arteries in patients before CAS was 6.68 ± 3.0Pa, 12.47 ± 5.98Pa, and 1.39 ± 0. 96Pa. WSS of the proximal, narrowest region, and distal carotid was 4.15 ± 1.42Pa, 6.71 ± 2.64Pa, and1.86 ± 1.13Pa one week after CAS, compared to 4.44 ± 1.91Pa, 7.90 ± 4.38Pa, and 2. 36 ± 1.09Pa six months after CAS. WSS of the proximal and narrowest region of the carotid artery was reduced after carotid stenting, and the difference was statistically significant (p < 0.001). There was no statistically significant difference in WSS between one week and six months after stenting (P > 0.05).
Conclusion: We employed early carotid WSS as a means of evaluating the efficacy of carotid artery stenting. Changes in carotid WSS are closely associated with carotid artery stenosis, providing valuable hemodynamic information for CAS treatment. This technique holds great application value in pre-operative evaluation and long-term follow-up.
Keywords: Carotid artery stenosis; Flow vector imaging; Ischemic stroke; Stenting; Wall shear stress.
© 2024 The Authors. Published by Elsevier Ltd.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
High-Frame Rate Vector Flow Imaging Technique: Initial Application in Evaluating the Hemodynamic Changes of Carotid Stenosis Caused by Atherosclerosis.Front Cardiovasc Med. 2021 Mar 8;8:617391. doi: 10.3389/fcvm.2021.617391. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 33763457 Free PMC article.
-
Analysis of restenosis after carotid artery stenting: preliminary results using computational fluid dynamics based on three-dimensional angiography.J Clin Neurosci. 2013 Nov;20(11):1582-7. doi: 10.1016/j.jocn.2013.03.042. Epub 2013 Sep 10. J Clin Neurosci. 2013. PMID: 24035423
-
Evaluation of Carotid Stenosis in a High-Stroke-Risk Population by Hemodynamic Dual-Parameters Based on Ultrasound Vector Flow Imaging.Brain Behav. 2024 Nov;14(11):e70150. doi: 10.1002/brb3.70150. Brain Behav. 2024. PMID: 39552116 Free PMC article.
-
Higher Risk for Reintervention in Patients after Stenting for Radiation-Induced Internal Carotid Artery Stenosis: A Single-Center Analysis and Systematic Review.Ann Vasc Surg. 2021 May;73:1-14. doi: 10.1016/j.avsg.2020.11.027. Epub 2020 Dec 26. Ann Vasc Surg. 2021. PMID: 33373766
-
Ultrasound surveillance after CAS and CEA: what's the evidence?J Cardiovasc Surg (Torino). 2014 Apr;55(2 Suppl 1):33-41. J Cardiovasc Surg (Torino). 2014. PMID: 24796896 Review.
References
-
- Goddi A., Bortolotto C., Raciti M.V., Fiorina I., Aiani L., Magistretti G., Sacchi A., Tinelli C., Calliada F. High-frame rate vector flow imaging of the carotid bifurcation in healthy adults: comparison with color Doppler imaging. J. Ultrasound Med. 2018;37(9):2263–2275. doi: 10.1002/jum.14579. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
