

Calcineurin inhibition rescues alloantigen-specific central memory T cell subsets that promote chronic GVHD
- PMID: 38828727
- PMCID: PMC11142741
- DOI: 10.1172/JCI170125
Calcineurin inhibition rescues alloantigen-specific central memory T cell subsets that promote chronic GVHD
Abstract
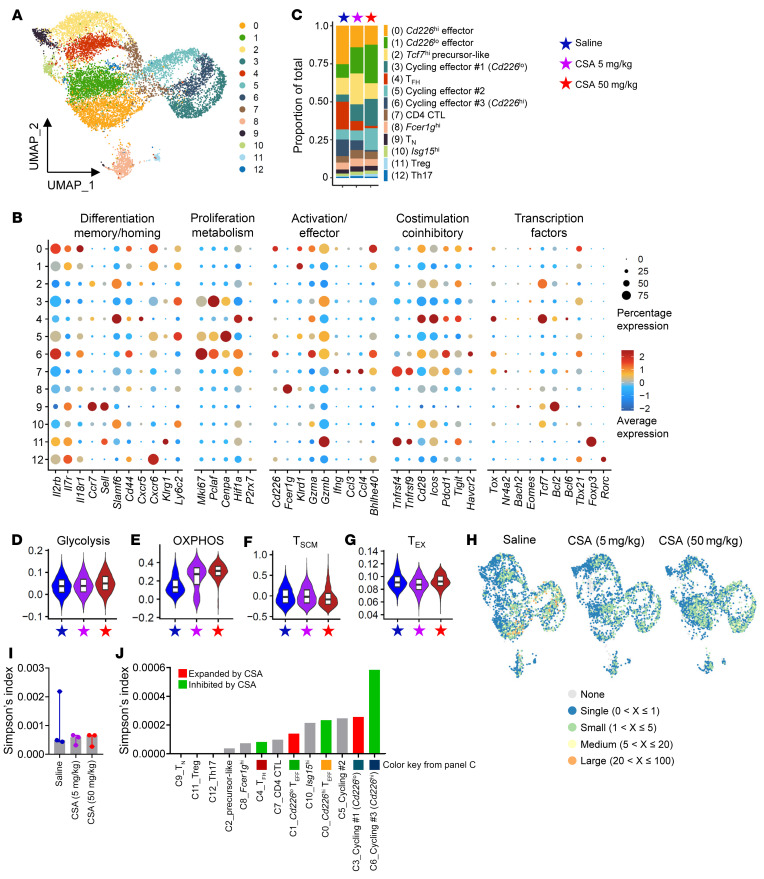
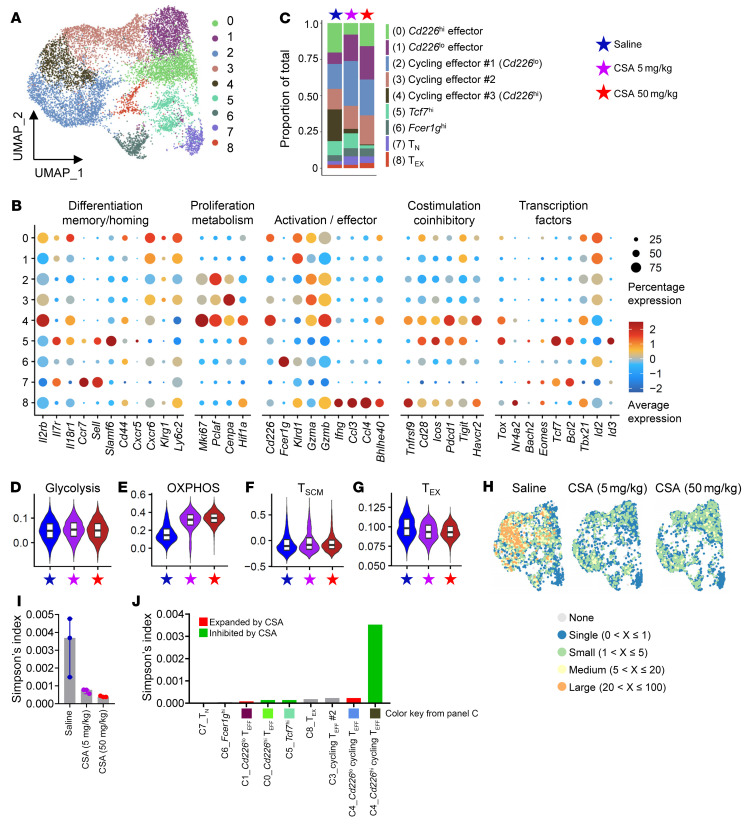
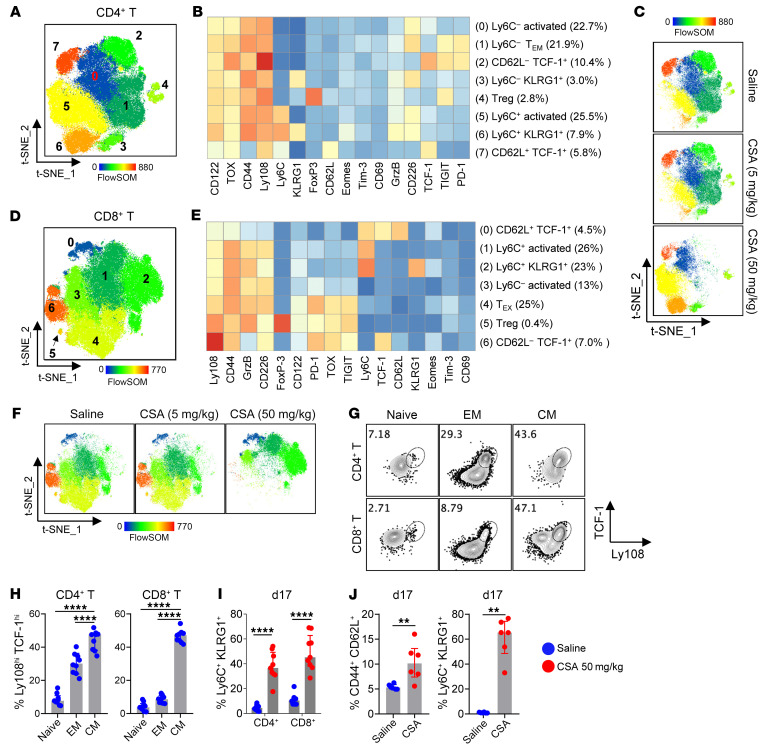
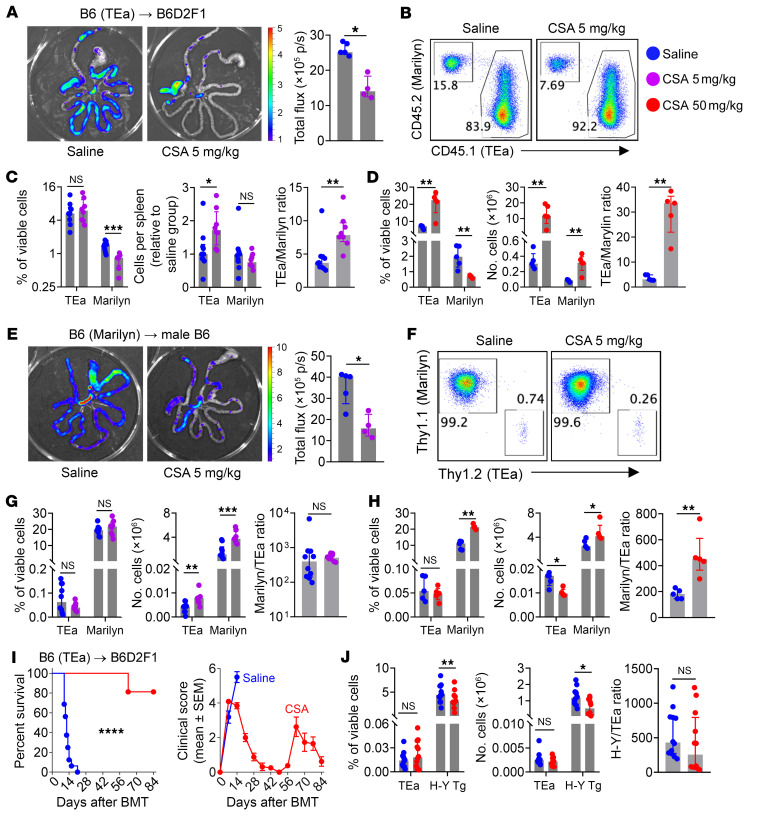
Calcineurin inhibitors (CNIs) constitute the backbone of modern acute graft-versus-host disease (aGVHD) prophylaxis regimens but have limited efficacy in the prevention and treatment of chronic GVHD (cGVHD). We investigated the effect of CNIs on immune tolerance after stem cell transplantation with discovery-based single-cell gene expression and T cell receptor (TCR) assays of clonal immunity in tandem with traditional protein-based approaches and preclinical modeling. While cyclosporin and tacrolimus suppressed the clonal expansion of CD8+ T cells during GVHD, alloreactive CD4+ T cell clusters were preferentially expanded. Moreover, CNIs mediated reversible dose-dependent suppression of T cell activation and all stages of donor T cell exhaustion. Critically, CNIs promoted the expansion of both polyclonal and TCR-specific alloreactive central memory CD4+ T cells (TCM) with high self-renewal capacity that mediated cGVHD following drug withdrawal. In contrast to posttransplant cyclophosphamide (PT-Cy), CSA was ineffective in eliminating IL-17A-secreting alloreactive T cell clones that play an important role in the pathogenesis of cGVHD. Collectively, we have shown that, although CNIs attenuate aGVHD, they paradoxically rescue alloantigen-specific TCM, especially within the CD4+ compartment in lymphoid and GVHD target tissues, thus predisposing patients to cGVHD. These data provide further evidence to caution against CNI-based immune suppression without concurrent approaches that eliminate alloreactive T cell clones.
Keywords: Bone marrow transplantation; Immunology; T cells; Transplantation.
Figures





References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
