

CNS Protective Effect of Selpercatinib in First-Line RET Fusion-Positive Advanced Non-Small Cell Lung Cancer
- PMID: 38828957
- PMCID: PMC11268557
- DOI: 10.1200/JCO.24.00724
CNS Protective Effect of Selpercatinib in First-Line RET Fusion-Positive Advanced Non-Small Cell Lung Cancer
Abstract
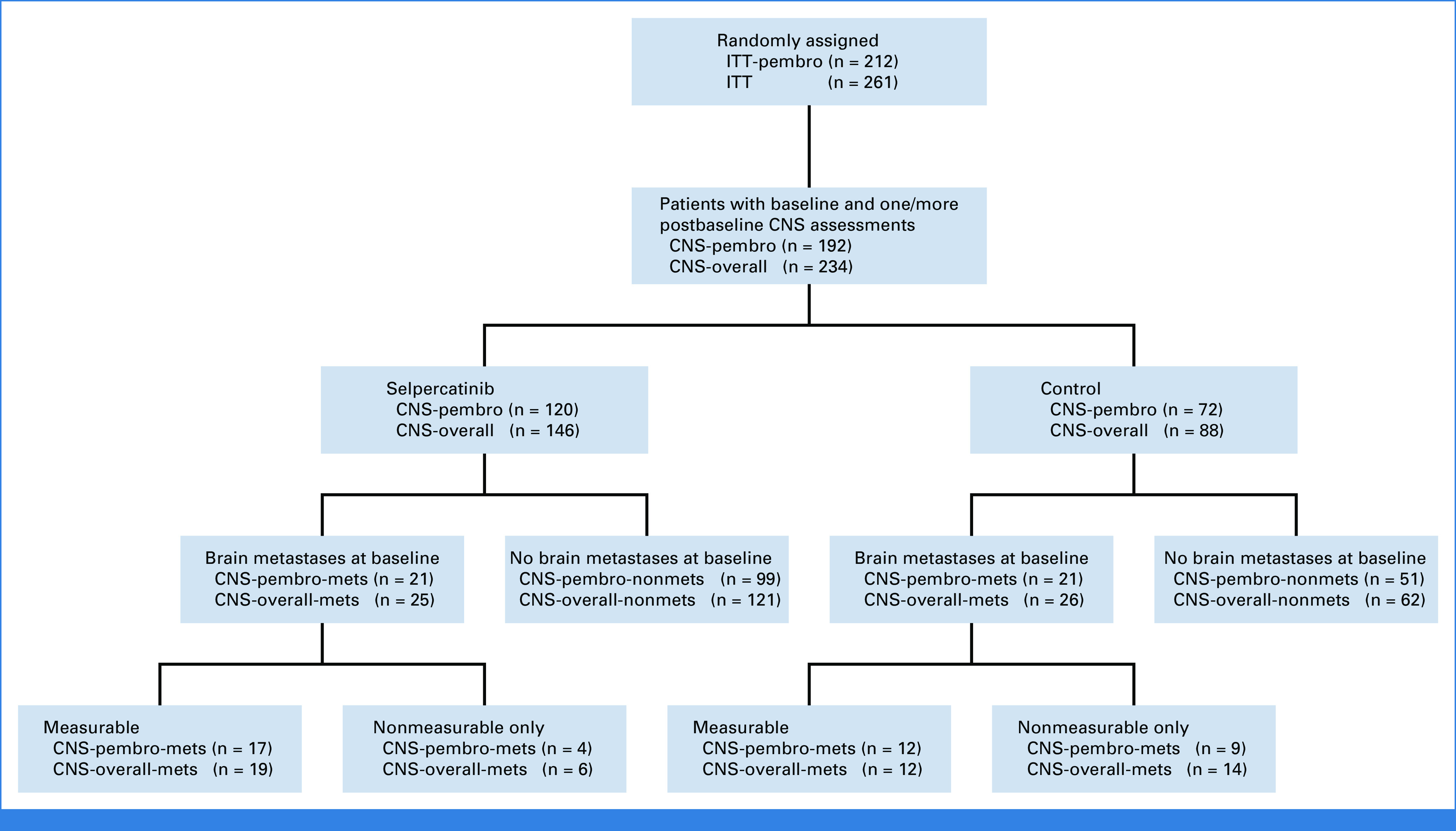
Clinical trials frequently include multiple end points that mature at different times. The initial report, typically based on the primary end point, may be published when key planned co-primary or secondary analyses are not yet available. Clinical Trial Updates provide an opportunity to disseminate additional results from studies, published in JCO or elsewhere, for which the primary end point has already been reported.Although the CNS activity of selpercatinib in patients with RET fusion-positive non-small cell lung cancer (NSCLC) has been previously described, the ability of potent RET inhibition to prevent new CNS metastases from developing has been challenging to measure without randomized data. Serial CNS scans were studied from LIBRETTO-431, a randomized phase III trial of selpercatinib versus platinum/pemetrexed ± pembrolizumab whose primary results have been previously disclosed. Intracranial outcomes were assessed by neuroradiologic blinded independent central review in patients with baseline and ≥1 postbaseline CNS scans. Of the 192 patients within the intention-to-treat pembrolizumab population with baseline CNS scans, 150 patients were without baseline CNS metastases. The cumulative incidence of CNS progression in these patients was reduced with selpercatinib versus chemotherapy + pembrolizumab (cause-specific hazard ratio [HR], 0.17 [95% CI, 0.04 to 0.69]). The HR for intracranial progression-free survival (PFS) was 0.46 (95% CI, 0.18 to 1.18). Among the 42 patients with baseline CNS metastases, similar trends were observed in the cumulative incidence of CNS progression (cause-specific HR, 0.61 [95% CI, 0.19 to 1.92]) and intracranial PFS (HR, 0.74 [95% CI, 0.28 to 1.97]). These data demonstrate that selpercatinib effectively treats existing CNS disease and prevents or delays the formation of new CNS metastases. These results reinforce the importance of identifying RET fusions in first-line patients with NSCLC and treating with selpercatinib.
Trial registration: ClinicalTrials.gov NCT04194944.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures





References
-
- Hendriks LE, Kerr KM, Menis J, et al. Oncogene-addicted metastatic non-small-cell lung cancer: ESMO clinical Practice guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023;34:339–357. - PubMed
-
- Jaiyesimi IA, Leighl NB, Ismaila N, et al. Therapy for stage IV non–small cell lung cancer with driver alterations: ASCO living guideline, version 2023.3. J Clin Oncol. 2024;42:e1–e22. - PubMed
-
- Reference deleted.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
