

Pneumocystis pneumonia in intensive care: clinical spectrum, prophylaxis patterns, antibiotic treatment delay impact, and role of corticosteroids. A French multicentre prospective cohort study
- PMID: 38829531
- PMCID: PMC11306648
- DOI: 10.1007/s00134-024-07489-2
Pneumocystis pneumonia in intensive care: clinical spectrum, prophylaxis patterns, antibiotic treatment delay impact, and role of corticosteroids. A French multicentre prospective cohort study
Abstract
Purpose: Severe Pneumocystis jirovecii pneumonia (PJP) requiring intensive care has been the subject of few prospective studies. It is unclear whether delayed curative antibiotic therapy may impact survival in these severe forms of PJP. The impact of corticosteroid therapy combined with antibiotics is also unclear.
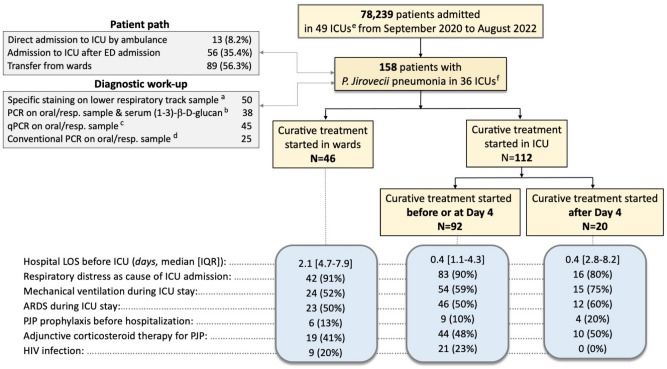
Methods: This multicentre, prospective observational study involving 49 adult intensive care units (ICUs) in France was designed to evaluate the severity, the clinical spectrum, and outcomes of patients with severe PJP, and to assess the association between delayed curative antibiotic treatment and adjunctive corticosteroid therapy with mortality.
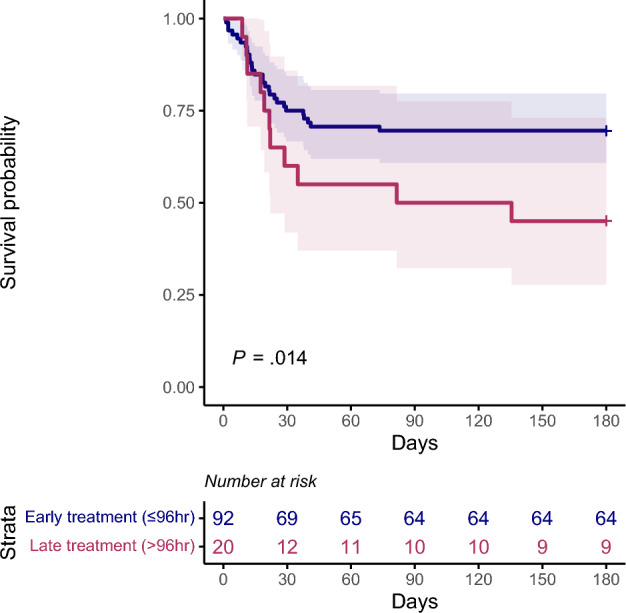
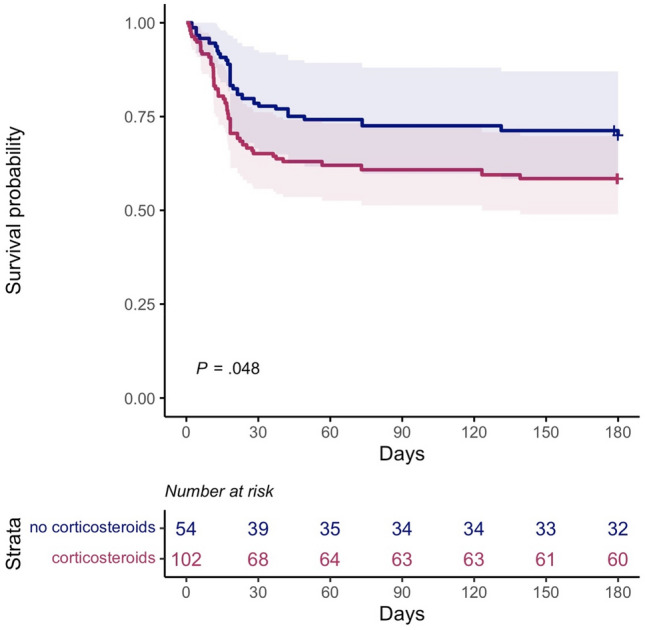
Results: We included 158 patients with PJP from September 2020 to August 2022. Their main reason for admission was acute respiratory failure (n = 150, 94.9%). 12% of them received antibiotic prophylaxis for PJP before ICU admission. The ICU, hospital, and 6-month mortality were 31.6%, 35.4%, and 40.5%, respectively. Using time-to-event analysis with a propensity score-based inverse probability of treatment weighting, the initiation of curative antibiotic treatment after 96 h of ICU admission was associated with faster occurrence of death [time ratio: 6.75; 95% confidence interval (95% CI): 1.48-30.82; P = 0.014]. The use of corticosteroids for PJP was associated with faster occurrence of death (time ratio: 2.48; 95% CI 1.01-6.08; P = 0.048).
Conclusion: This study showed that few patients with PJP admitted to intensive care received prophylactic antibiotic therapy, that delay in curative antibiotic treatment was common and that both delay in curative antibiotic treatment and adjunctive corticosteroids for PJP were associated with accelerated mortality.
Keywords: Pneumocystis jirovecii; Adjunctive corticosteroid therapy; Delayed treatment; Intensive care; Mortality; Prophylaxis.
© 2024. The Author(s).
Conflict of interest statement
There are no competing interests for any author concerning the submitted work.
Figures
References
-
- Grønseth S, Rogne T, Hannula R, Åsvold BO, Afset JE, Damås JK (2021) Epidemiological and clinical characteristics of immunocompromised patients infected with Pneumocystis jirovecii in a twelve-year retrospective study from Norway. BMC Infect Dis 21:659. 10.1186/s12879-021-06144-1 10.1186/s12879-021-06144-1 - DOI - PMC - PubMed
-
- Kolbrink B, Scheikholeslami-Sabzewari J, Borzikowsky C, von Samson- Himmelstjerna FA, Ullmann AJ, Kunzendorf U (2022) Schulte K (2022) Evolving epidemiology of pneumocystis pneumonia: findings from a longitudinal population-based study and a retrospective multi-center study in Germany. Lancet Reg Health Eur 18:100400. 10.1016/j.lanepe.2022.100400 10.1016/j.lanepe.2022.100400 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
