

Jinlida for Diabetes Prevention in Impaired Glucose Tolerance and Multiple Metabolic Abnormalities: The FOCUS Randomized Clinical Trial
- PMID: 38829648
- PMCID: PMC11148787
- DOI: 10.1001/jamainternmed.2024.1190
Jinlida for Diabetes Prevention in Impaired Glucose Tolerance and Multiple Metabolic Abnormalities: The FOCUS Randomized Clinical Trial
Erratum in
-
Change to Open Access.JAMA Intern Med. 2024 Sep 1;184(9):1137. doi: 10.1001/jamainternmed.2024.3409. JAMA Intern Med. 2024. PMID: 38976281 Free PMC article. No abstract available.
-
Errors in Results Section and Figure 3.JAMA Intern Med. 2024 Oct 1;184(10):1270. doi: 10.1001/jamainternmed.2024.4669. JAMA Intern Med. 2024. PMID: 39226038 Free PMC article. No abstract available.
Abstract
Importance: Previous studies have shown that Jinlida (JLD) granules, an approved treatment for type 2 diabetes in China, can reduce blood glucose level, reduce glycated hemoglobin (HbA1c), and improve insulin resistance in people with type 2 diabetes.
Objective: To evaluate the effect of long-term administration of JLD vs placebo on the incidence of diabetes in participants with impaired glucose tolerance (IGT) and multiple metabolic abnormalities.
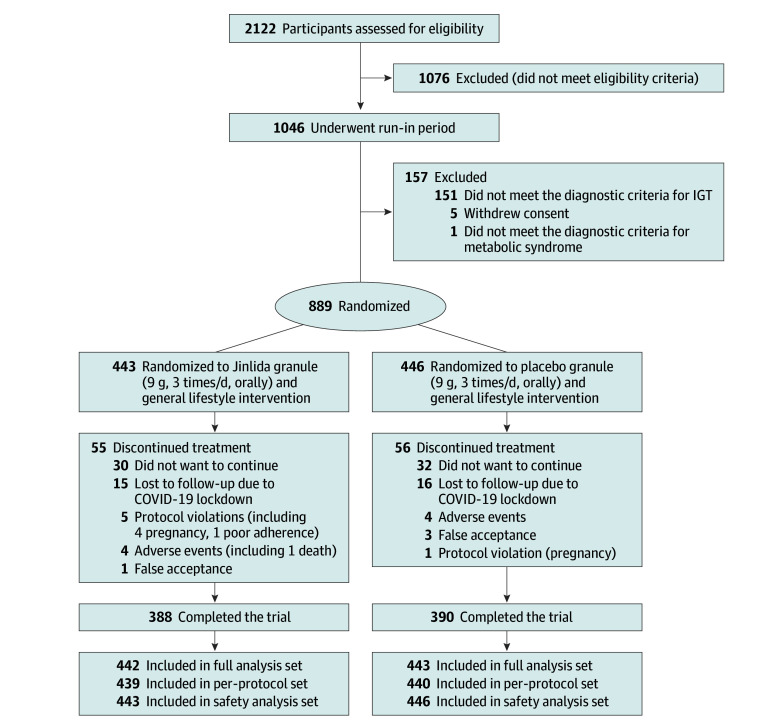
Design, setting, and participants: This multicenter, double-blind, placebo-controlled randomized clinical trial (FOCUS) was conducted across 35 centers in 21 cities in China from June 2019 to February 2023. Individuals aged 18 to 70 years with IGT and multiple metabolic abnormalities were enrolled.
Intervention: Participants were randomly allocated 1:1 to receive JLD or placebo (9 g, 3 times per day, orally). They continued this regimen until they developed diabetes, withdrew from the study, were lost to follow-up, or died.
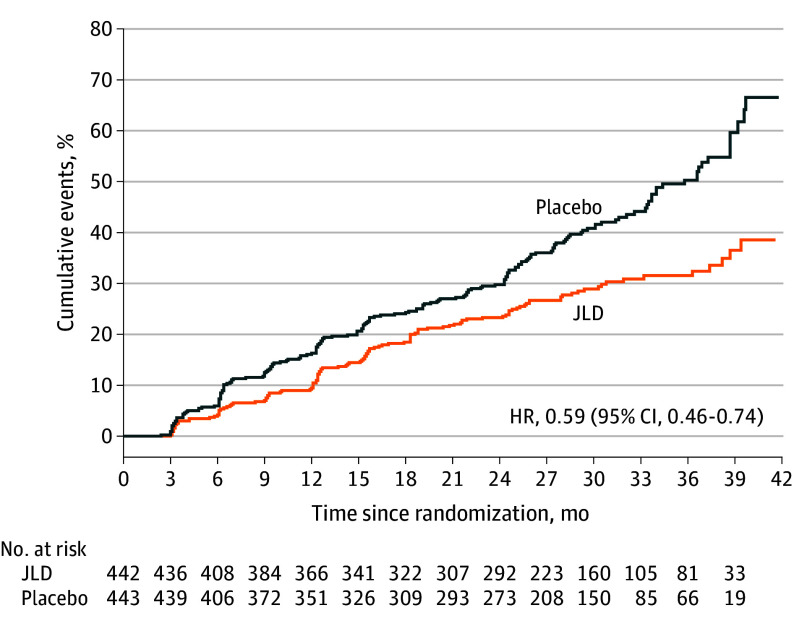
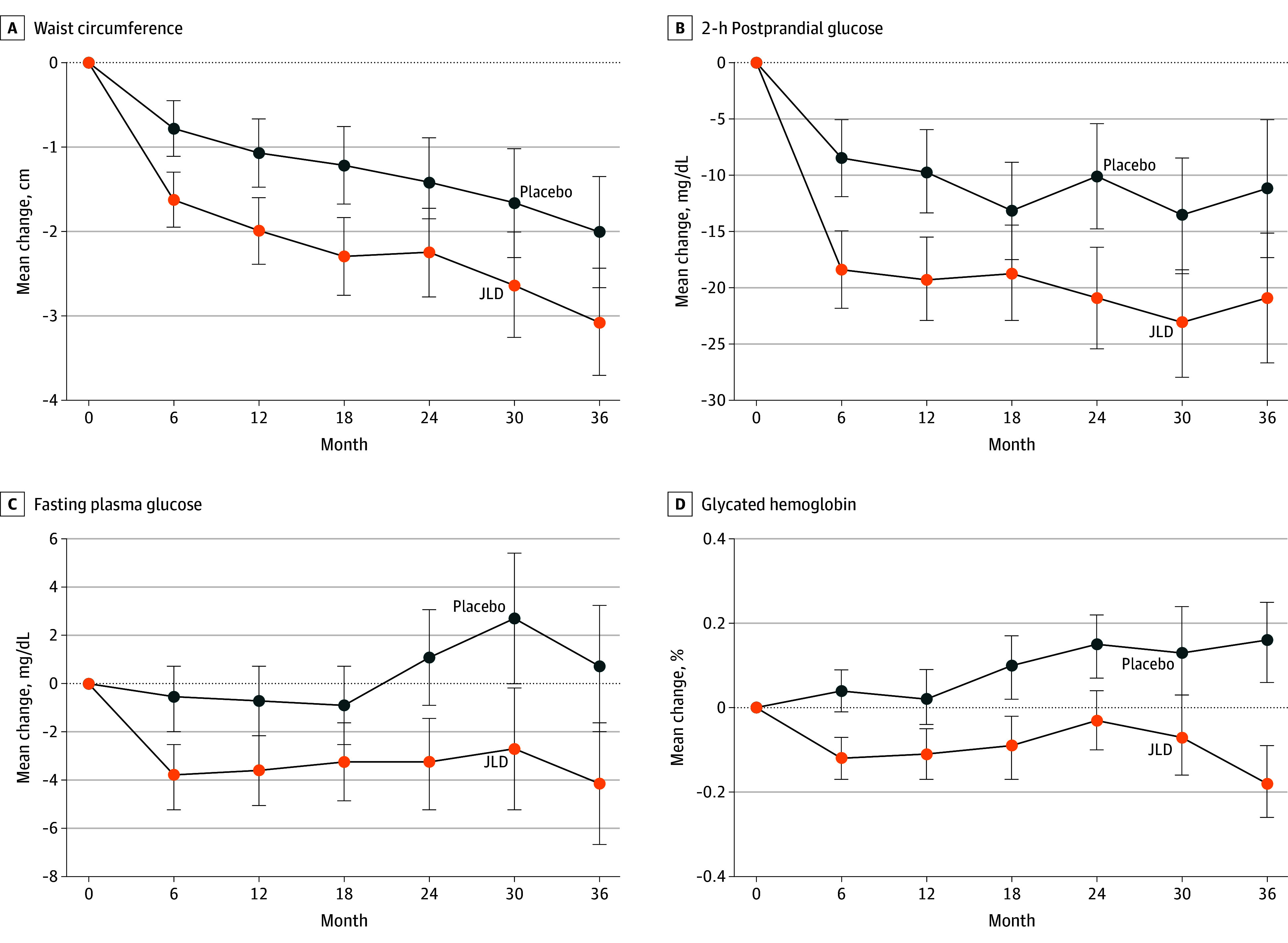
Main outcomes and measures: The primary outcome was the occurrence of diabetes, which was determined by 2 consecutive oral glucose tolerance tests. Secondary outcomes included waist circumference; fasting and 2-hour postprandial plasma glucose levels; HbA1c; fasting insulin level; homeostatic model assessment for insulin resistance (HOMA-IR); total cholesterol, low-density lipoprotein cholesterol, and triglyceride levels; ankle-brachial index; and carotid intima-media thickness.
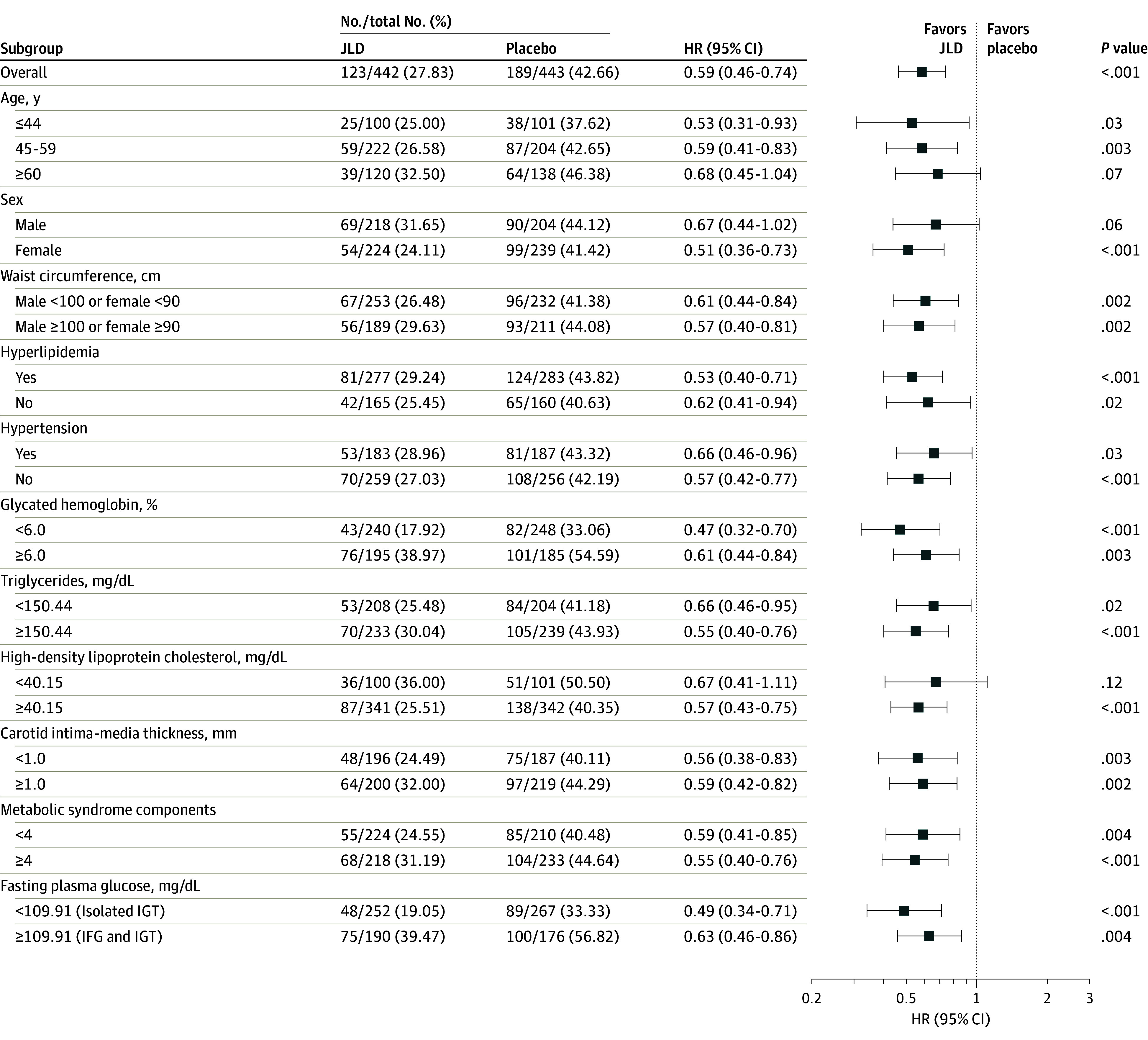
Results: A total of 889 participants were randomized, of whom 885 were in the full analysis set (442 in the JLD group; 443 in the placebo group; mean [SD] age, 52.57 [10.33] years; 463 [52.32%] female). Following a median observation period of 2.20 years (IQR, 1.27-2.64 years), participants in the JLD group had a lower risk of developing diabetes compared with those in the placebo group (hazard ratio, 0.59; 95% CI, 0.46-0.74; P < .001). During the follow-up period, the JLD group had a between-group difference of 0.95 cm (95% CI, 0.36-1.55 cm) in waist circumference, 9.2 mg/dL (95% CI, 5.4-13.0 mg/dL) in 2-hour postprandial blood glucose level, 3.8 mg/dL (95% CI, 2.2-5.6 mg/dL) in fasting blood glucose level, 0.20% (95% CI, 0.13%-0.27%) in HbA1c, 6.6 mg/dL (95% CI, 1.9-11.2) in total cholesterol level, 4.3 mg/dL (95% CI, 0.8-7.7 mg/dL) in low-density lipoprotein cholesterol level, 25.7 mg/dL (95% CI, 15.9-35.4 mg/dL) in triglyceride levels, and 0.47 (95% CI, 0.12-0.83) in HOMA-IR compared with the placebo group. After 24 months of follow-up, the JLD group had a significant improvement in ankle-brachial index and waist circumference compared with the placebo group.
Conclusions and relevance: The findings suggest that JLD can reduce the risk of diabetes in participants with IGT and multiple metabolic abnormalities.
Trial registration: Chinese Clinical Trial Register: ChiCTR1900023241.
Conflict of interest statement
Figures
Comment on
-
Traditional Chinese Medicine to Prevent Type 2 Diabetes-A Difficult Path Forward.JAMA Intern Med. 2024 Jul 1;184(7):736. doi: 10.1001/jamainternmed.2024.1208. JAMA Intern Med. 2024. PMID: 38829623 No abstract available.
References
-
- Gerstein HC, Yusuf S, Bosch J, et al. ; DREAM (Diabetes REduction Assessment with ramipril and rosiglitazone Medication) Trial Investigators . Effect of rosiglitazone on the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: a randomised controlled trial. Lancet. 2006;368(9541):1096-1105. doi:10.1016/S0140-6736(06)69420-8 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
