

Specific pelvic shape in patients with developmental dysplasia of the hip on 3D morphometric homologous model analysis
- PMID: 38829863
- PMCID: PMC11146717
- DOI: 10.1371/journal.pone.0300938
Specific pelvic shape in patients with developmental dysplasia of the hip on 3D morphometric homologous model analysis
Abstract
Purpose: To clarify the morphological factors of the pelvis in patients with developmental dysplasia of the hip (DDH), three-dimensional (3D) pelvic morphology was analyzed using a template-fitting technique.
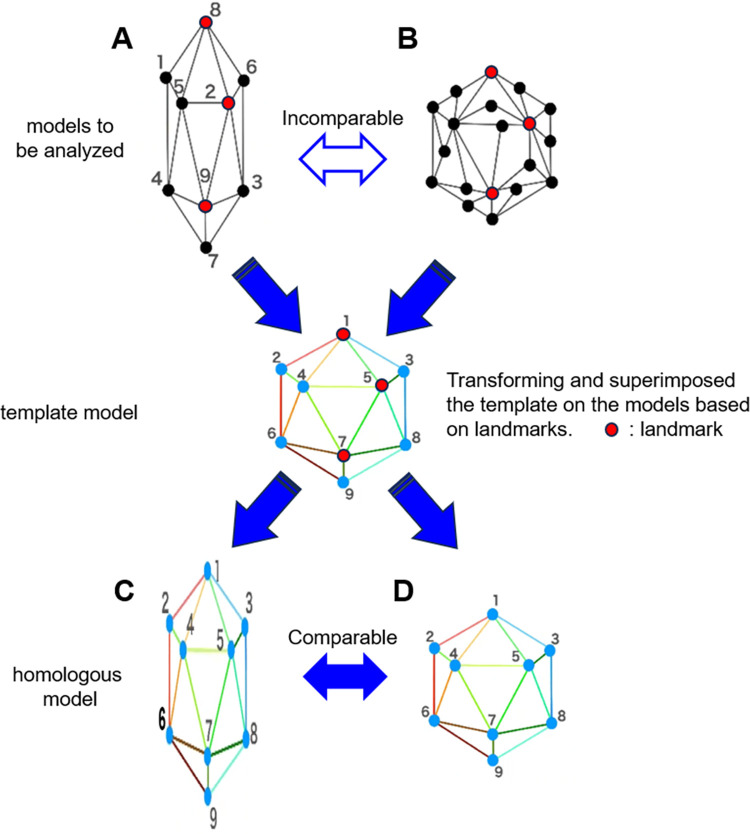
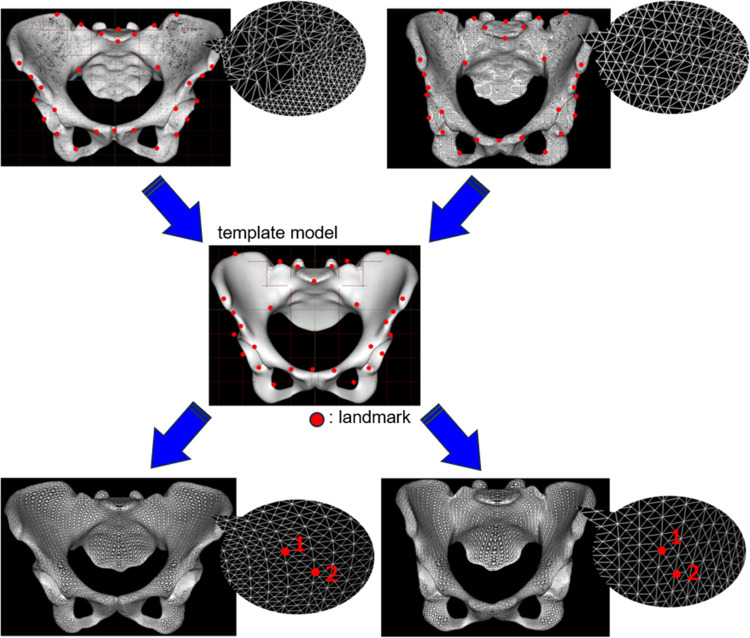
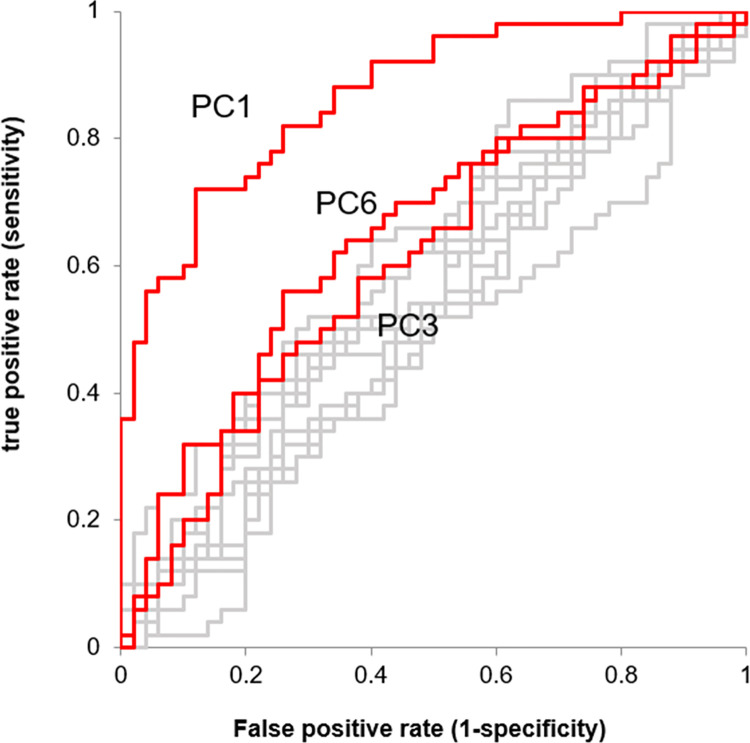
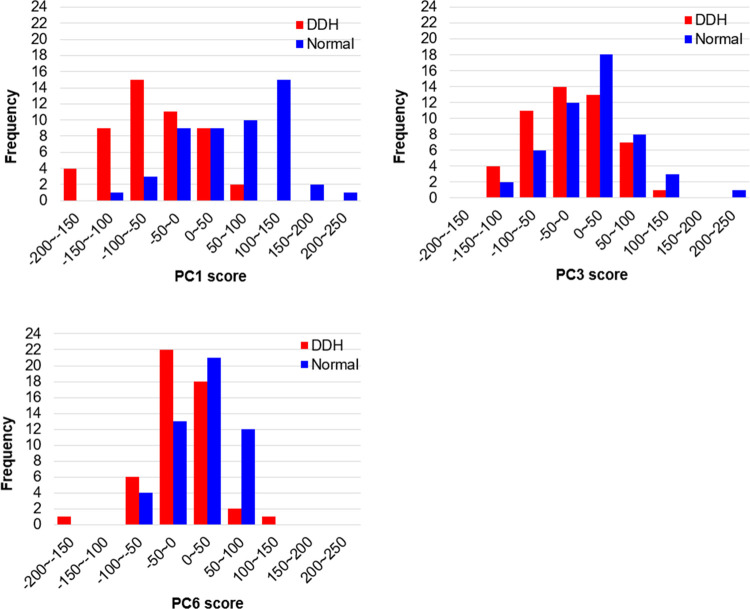
Methods: Three-dimensional pelvic data of 50 patients with DDH (DDH group) and 3D pelvic data of 50 patients without obvious pelvic deformity (Normal group) were used. All patients were female. A template model was created by averaging the normal pelvises into a symmetrical and isotropic mesh. Next, 100 homologous models were generated by fitting the pelvic data of each group of patients to the template model. Principal component analysis was performed on the coordinates of each vertex (15,235 vertices) of the pelvic homologous model. In addition, a receiver-operating characteristic (ROC) curve was calculated from the sensitivity of DDH positivity for each principal component, and principal components for which the area under the curve was significantly large were extracted (p<0.05). Finally, which components of the pelvic morphology frequently seen in DDH patients are related to these extracted principal components was evaluated.
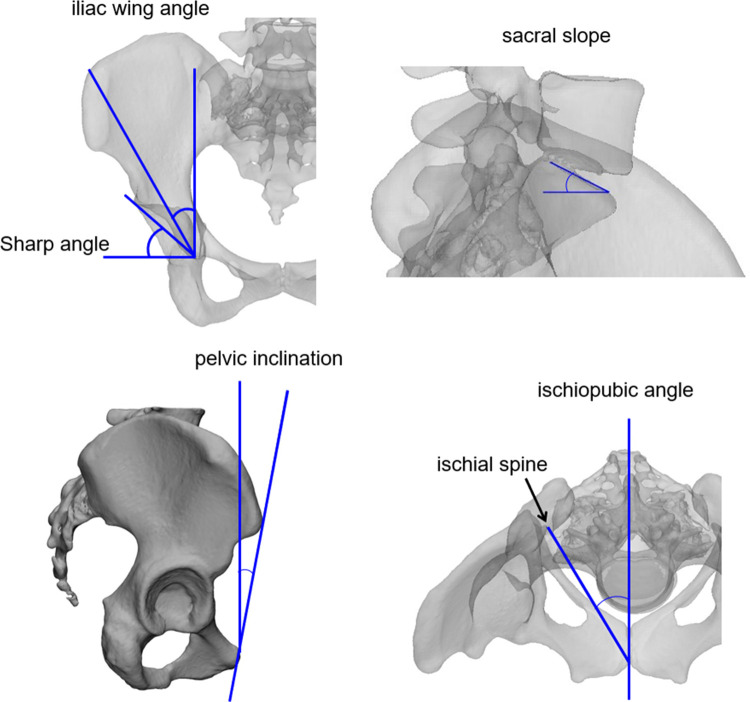
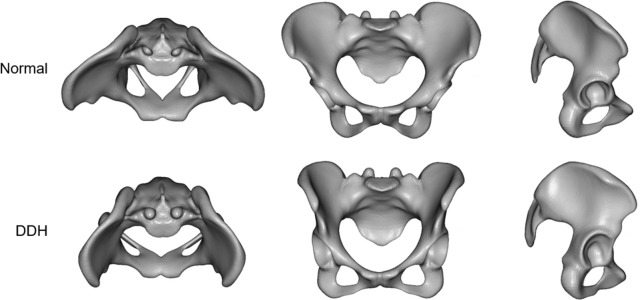
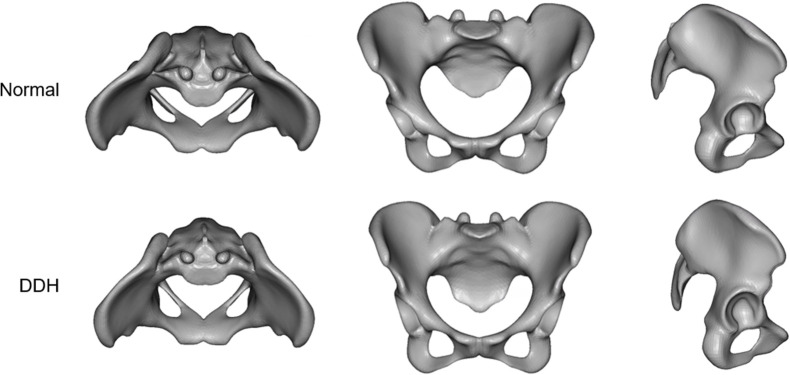
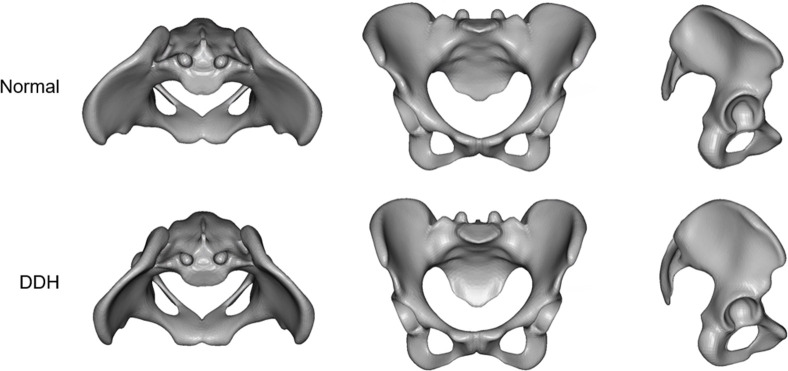
Results: The first, third, and sixth principal components showed significantly larger areas under the ROC curves. The morphology indicated by the first principal component was associated with a decrease in coxal inclination in both the coronal and horizontal planes. The third principal component was related to the sacral inclination in the sagittal plane. The sixth principal component was associated with narrowing of the superior part of the pelvis.
Conclusion: The most important factor in the difference between normal and DDH pelvises was the change in the coxal angle in both the coronal and horizontal planes. That is, in the anterior and superior views, the normal pelvis is a triangle, whereas in DDH, it was more like a quadrilateral.
Copyright: © 2024 Sasaki et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Wiberg G. Studies on dysplastic acetabula and congenital subluxation of the hip joint with special reference to the complication of osteoarthritis. Stockholm: Exp., Norstedt Stockholm; 1939.
-
- Jingushi S, Ohfuji S, Sofue M, Hirota Y, Itoman M, Matsumoto T, et al. Multiinstitutional epidemiological study regarding osteoarthritis of the hip in Japan. Journal of orthopaedic science: official journal of the Japanese Orthopaedic Association. 2010;15(5):626–31. doi: 10.1007/s00776-010-1507-8 . - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
