

Safety and effectiveness of remdesivir in hospitalized patients with COVID-19 and severe renal impairment: experience at a large medical center
- PMID: 38830017
- PMCID: PMC11149583
- DOI: 10.1080/07853890.2024.2361843
Safety and effectiveness of remdesivir in hospitalized patients with COVID-19 and severe renal impairment: experience at a large medical center
Abstract
Background: Literature on the safety of remdesivir in hospitalized COVID-19 patients with severe renal impairment is limited. We aimed to investigate the safety and effectiveness of remdesivir in this population.
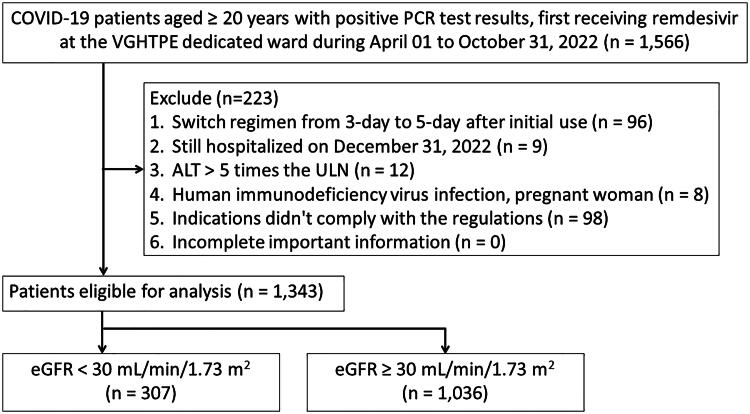
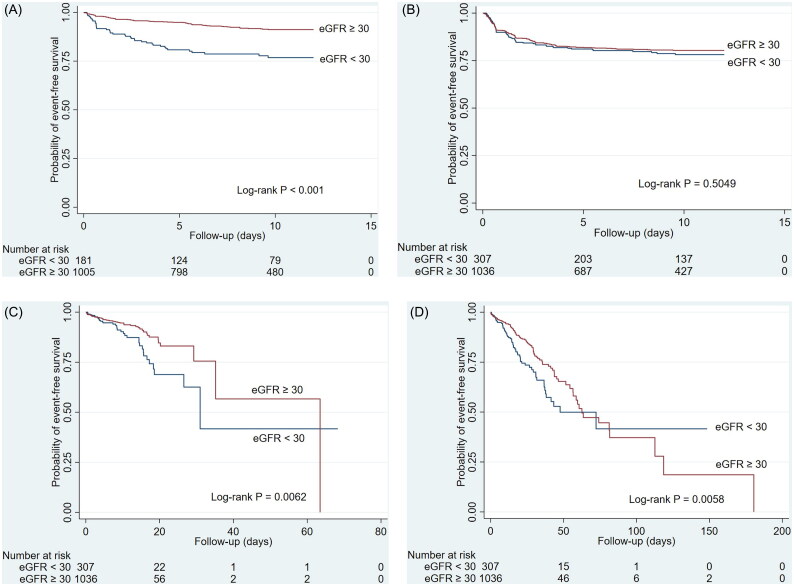
Methods: We conducted a retrospective cohort study of adult hospitalized COVID-19 patients who received remdesivir between April 2022 and October 2022. Outcomes were compared between estimated glomerular filtration rate (eGFR) <30 mL/min/1.73 m2 and ≥30 mL/min/1.73 m2 groups. The primary safety outcomes were acute kidney injury (AKI) and bradycardia, while the primary effectiveness outcomes included mortality in COVID-19-dedicated wards and hospital mortality. Secondary outcomes included laboratory changes, disease progression, and recovery time.
Results: A total of 1,343 patients were recruited, with 307 (22.9%) in the eGFR <30 group and 1,036 (77.1%) in the eGFR ≥30 group. Patients with an eGFR <30 had higher risks of AKI (adjusted hazard ratio [aHR] 2.92, 95% CI 1.93-4.44) and hospital mortality (aHR 1.47, 95% CI 1.06-2.05) but had comparable risks of bradycardia (aHR 1.15, 95% CI 0.85-1.56) and mortality in dedicated wards (aHR 1.43, 95% CI 0.90-2.28) than patients with an eGFR ≥30. Risk of disease progression was higher in the eGFR <30 group (adjusted odds ratio 1.62, 95% CI 1.16-2.26). No difference between the two groups in laboratory changes and recovery time.
Conclusions: Hospitalized COVID-19 patients receiving remdesivir with severe renal impairment had an increased risk of AKI, hospital mortality, and COVID-19 disease progression compared to patients without severe renal impairment.
Keywords: COVID-19; acute kidney injury; remdesivir; severe renal impairment.
Conflict of interest statement
The authors report no conflict of interest.
Figures
Similar articles
-
Clinical outcomes and safety of remdesivir in hospitalized individuals with COVID-19, with or without severe renal impairment.J Infect Public Health. 2024 Jul;17(7):102460. doi: 10.1016/j.jiph.2024.05.048. Epub 2024 May 24. J Infect Public Health. 2024. PMID: 38820894
-
Remdesivir, Renal Function and Short-Term Clinical Outcomes in Elderly COVID-19 Pneumonia Patients: A Single-Centre Study.Clin Interv Aging. 2021 Jun 3;16:1037-1046. doi: 10.2147/CIA.S313028. eCollection 2021. Clin Interv Aging. 2021. PMID: 34113086 Free PMC article.
-
Efficacy and Safety of Remdesivir in People With Impaired Kidney Function Hospitalized for COVID-19 Pneumonia: A Randomized Clinical Trial.Clin Infect Dis. 2024 Nov 22;79(5):1172-1181. doi: 10.1093/cid/ciae333. Clin Infect Dis. 2024. PMID: 38913574 Free PMC article. Clinical Trial.
-
Remdesivir for the treatment of COVID 19: review of the pharmacological properties, safety and clinical effectiveness.Expert Opin Drug Saf. 2021 Nov;20(11):1299-1307. doi: 10.1080/14740338.2021.1962284. Epub 2021 Aug 16. Expert Opin Drug Saf. 2021. PMID: 34338121 Review.
-
Remdesivir for Adults With COVID-19 : A Living Systematic Review for American College of Physicians Practice Points.Ann Intern Med. 2021 Feb;174(2):209-220. doi: 10.7326/M20-5752. Epub 2020 Oct 5. Ann Intern Med. 2021. Update in: Ann Intern Med. 2021 May;174(5):663-672. doi: 10.7326/M20-8148. PMID: 33017170 Free PMC article. Updated.
Cited by
-
Unlocking the potential of remdesivir: innovative approaches to drug delivery.Drug Deliv Transl Res. 2025 Apr 17. doi: 10.1007/s13346-025-01843-7. Online ahead of print. Drug Deliv Transl Res. 2025. PMID: 40244526 Review.
-
Safety evaluation of remdesivir administration in patients with severe renal impairment and coronavirus disease: a systematic review and meta-analysis.BMC Infect Dis. 2025 Jun 2;25(1):782. doi: 10.1186/s12879-025-11153-5. BMC Infect Dis. 2025. PMID: 40457282 Free PMC article.
References
-
- World Health Organization. WHO Coronavirus (COVID-19). Dashboard. https://covid19.who.int/. (accessed October, 7 2023).
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous