

Identification and validation of a blood- based diagnostic lipidomic signature of pediatric inflammatory bowel disease
- PMID: 38830848
- PMCID: PMC11148148
- DOI: 10.1038/s41467-024-48763-7
Identification and validation of a blood- based diagnostic lipidomic signature of pediatric inflammatory bowel disease
Abstract
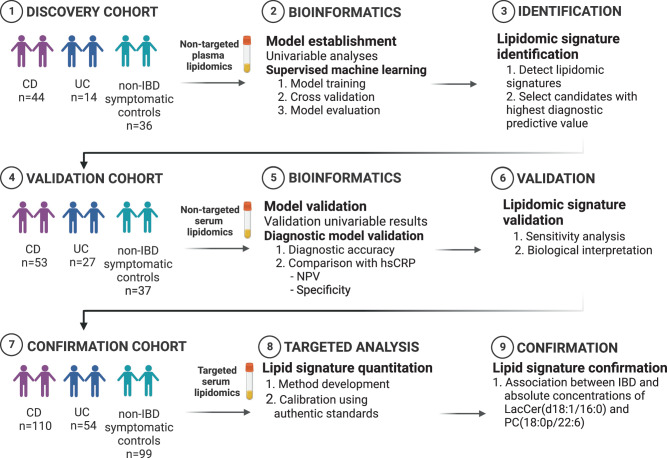
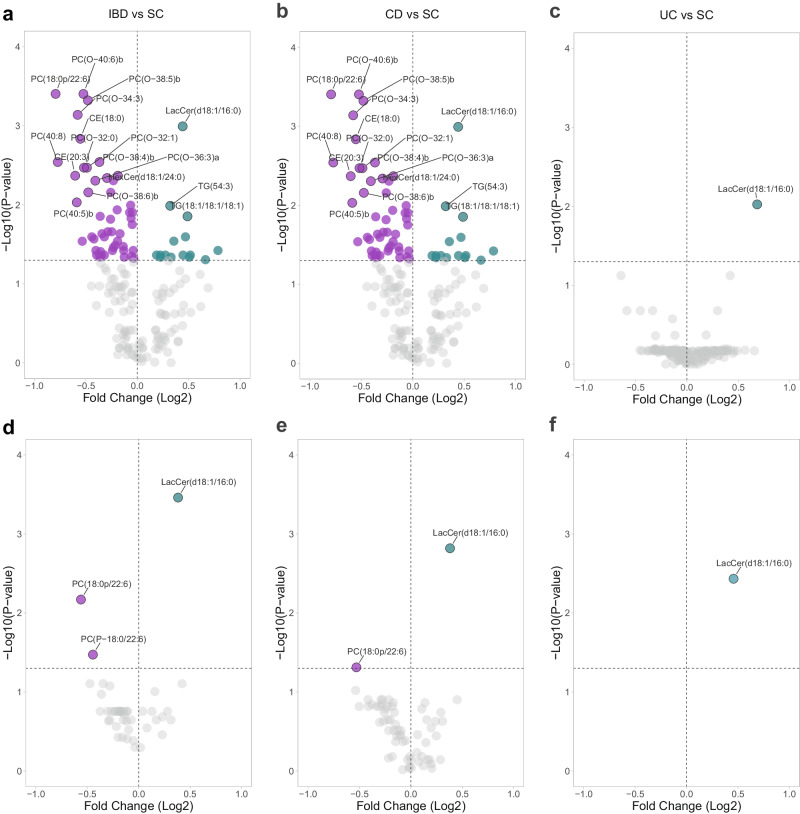
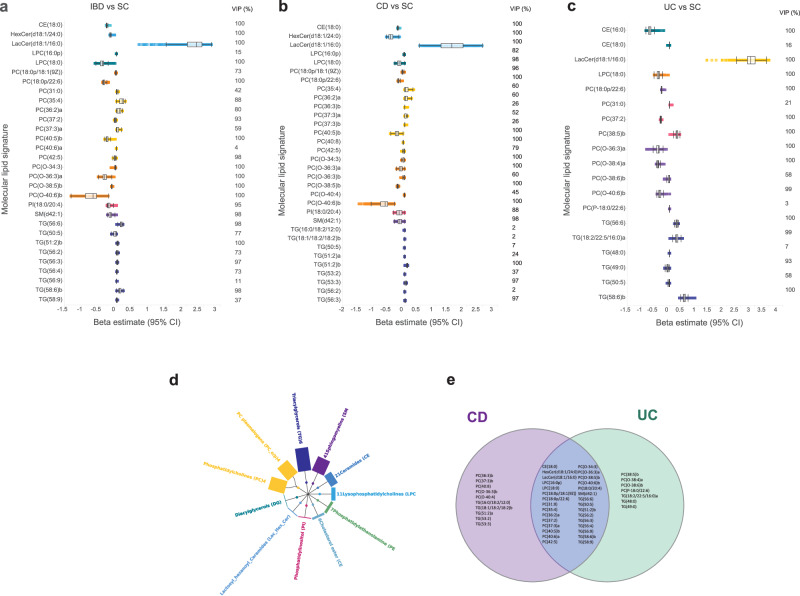
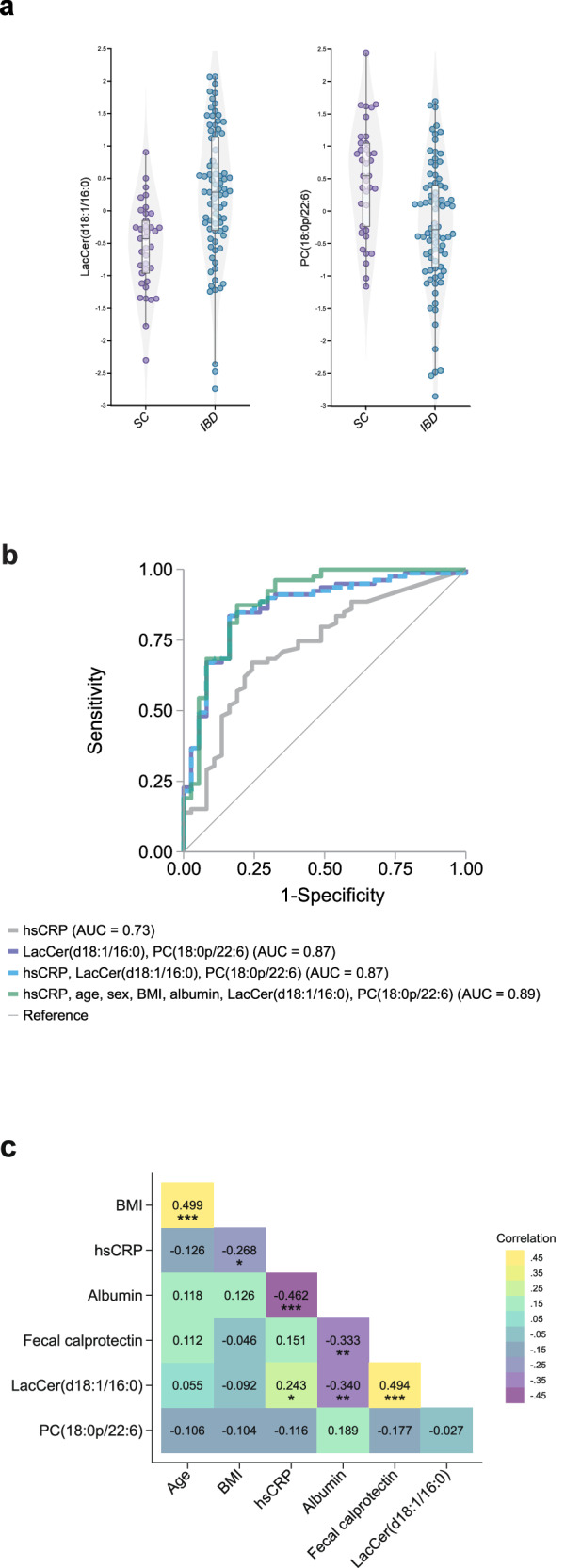
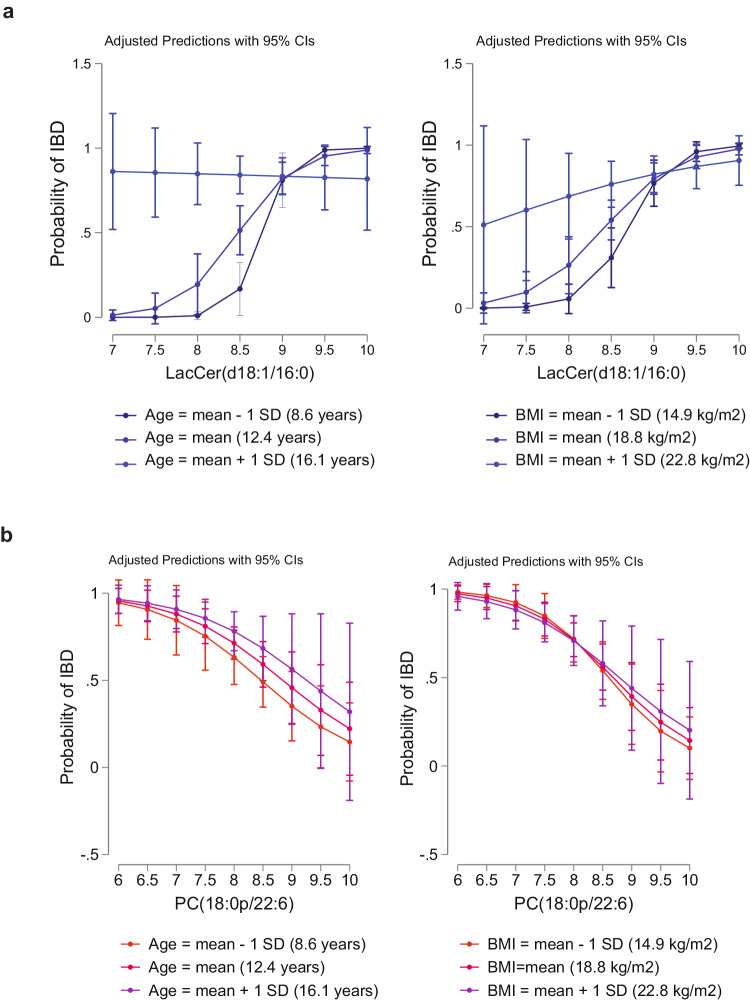
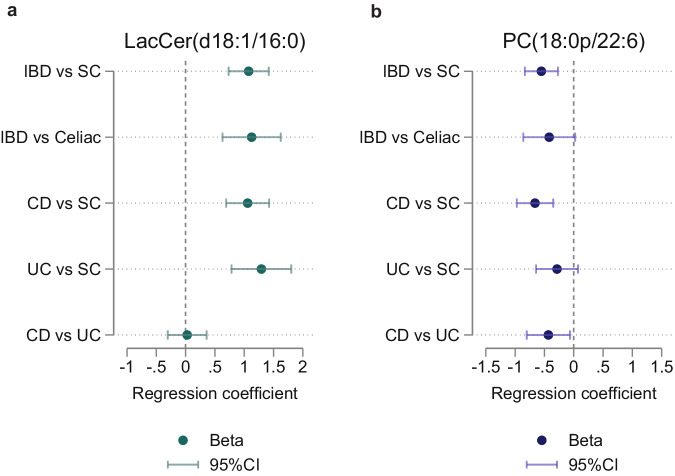
Improved biomarkers are needed for pediatric inflammatory bowel disease. Here we identify a diagnostic lipidomic signature for pediatric inflammatory bowel disease by analyzing blood samples from a discovery cohort of incident treatment-naïve pediatric patients and validating findings in an independent inception cohort. The lipidomic signature comprising of only lactosyl ceramide (d18:1/16:0) and phosphatidylcholine (18:0p/22:6) improves the diagnostic prediction compared with high-sensitivity C-reactive protein. Adding high-sensitivity C-reactive protein to the signature does not improve its performance. In patients providing a stool sample, the diagnostic performance of the lipidomic signature and fecal calprotectin, a marker of gastrointestinal inflammation, does not substantially differ. Upon investigation in a third pediatric cohort, the findings of increased lactosyl ceramide (d18:1/16:0) and decreased phosphatidylcholine (18:0p/22:6) absolute concentrations are confirmed. Translation of the lipidomic signature into a scalable diagnostic blood test for pediatric inflammatory bowel disease has the potential to support clinical decision making.
© 2024. The Author(s).
Conflict of interest statement
Dr Salihovic has no conflicts of interest to disclose. Dr Nyström has served as speaker and/or advisory board member for Abigo, Baxter, Ferring, Fresenius-Kabi, Mylan/Meda, Nutricia, Shire, Takeda, Thermo Fisher Scientific, Tillotts Pharma, and Viatris. Dr Bache-Wiig Mathisen has served as advisory board member for Tillotts Pharma. Dr Andersen has no conflicts of interest to disclose. Dr Olbjørn has no conflicts of interest to disclose. Dr Perminow has served as a speaker and/or advisory borad member for AbbVie. She has also received grant support from Ferring, Tillotts Pharma and Takeda. Dr Opheim has no conflicts of interest to disclose. Dr. Detlie has served as a speaker, consultant, or advisory board member for AbbVie, Ferring, Pfizer, Pharmacosmos, Tillotts, and Vifor Pharma. He has received unrestricted research grants from AbbVie, and Pharmacosmos. Dr Huppertz-Hauss has no conflicts of interest to disclose. Dr Bazov has no conflicts of interest to disclose. Dr Kruse has no conflicts of interest to disclose. Dr Lindqvist has no conflicts of interest to disclose. Dr. C. R. H. Hedin has received speaker fees from Takeda, Ferring, AbbVie, and Janssen, and consultancy fees from Pfizer. She has acted as local principal investigator for clinical trials for Janssen and GlaxoSmithKline. She is PI on projects at the Karolinska Institutet partly funded by investigator-initiated grants from Takeda and Tillotts. None of these activities have any relation to the present study. Dr Carlson has received speaker’s fees from ViforPharma. She is the national PI for clinical trials for AstraZeneca. None of these activities have any relation to the present study. Dr Öhman has received financial support for research from Genetic Analysis A.S., Biocodex, Danone Research and AstraZeneca and served as Consultant/Advisory Board member for Genetic Analysis A.S., and as a speaker for Biocodex, Janssen, Ferring Pharmaceuticals, Takeda, AbbVie, Novartis, Avanos, and MEDA. Dr Magnusson has no conflicts of interest to disclose. Dr Keita has no conflicts of interest to disclose. Dr Söderholm has no conflicts of interest to disclose. Dr D’Amato has received unrestricted research grants and serves as consultant for QOL Medical. Dr Orešič has no conflicts of interest to disclose. Dr Noble has no conflicts of interest to disclose. Dr Satsangi has consultancy fees from Janssen. Current research support from The Helmsley Trust, CCUK, and EC Horizon 2020 programme. Dr Uhlig has received research support or consultancy fees from Janssen, UCB Pharma, Eli Lilly, Boehringer Ingelheim, Pfizer, AbbVie, BMS Celgene, GSK, OMass and MiroBio. Dr Dorn-Rasmussen has no conflicts of interest to disclose. Dr Wewer has no conflicts of interest to disclose. Dr Burisch reports personal fees from AbbVie, Celgene, Pfizer, Samsung Bioepis, Pharmacosmos, Ferring, and Galapagos; grants and personal fees from Janssen, MSD, Takeda, Tillots Pharma, and Bristol Myers Squibb; and grants from Novo Nordisk. Dr Repsilber has no conflicts of interest to disclose. Dr Hyötyläinen has no conflicts of interest to disclose. Dr Høivik has served as a speaker and/or advisory board member for AbbVie, Ferring, Galapagos, MEDA, MSD, Pfizer, Takeda, and Tillotts Pharma. She has also received grant support from Ferring, Tillotts Pharma, Takeda, and Pfizer. Dr Halfvarson has served as speaker and/or advisory board member for AbbVie, Aqilion, BMS, Celgene, Celltrion, Dr Falk Pharma and the Falk Foundation, Ferring, Galapagos, Gilead, Hospira, Index Pharma, Janssen, MEDA, Medivir, MSD, Novartis, Pfizer, Prometheus Laboratories Inc., Sandoz, Shire, Takeda, Thermo Fisher Scientific, Tillotts Pharma, Vifor Pharma, UCB and received grant support from Janssen, MSD and Takeda.
Figures
References
-
- Malham M, et al. Paediatric onset inflammatory bowel disease is a distinct and aggressive phenotype—a comparative population-based study. GastroHep. 2019;1:266–273. doi: 10.1002/ygh2.368. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
