

A global consensus on the definitions, diagnosis and management of fibrostenosing small bowel Crohn's disease in clinical practice
- PMID: 38831007
- PMCID: PMC12063211
- DOI: 10.1038/s41575-024-00935-y
A global consensus on the definitions, diagnosis and management of fibrostenosing small bowel Crohn's disease in clinical practice
Abstract
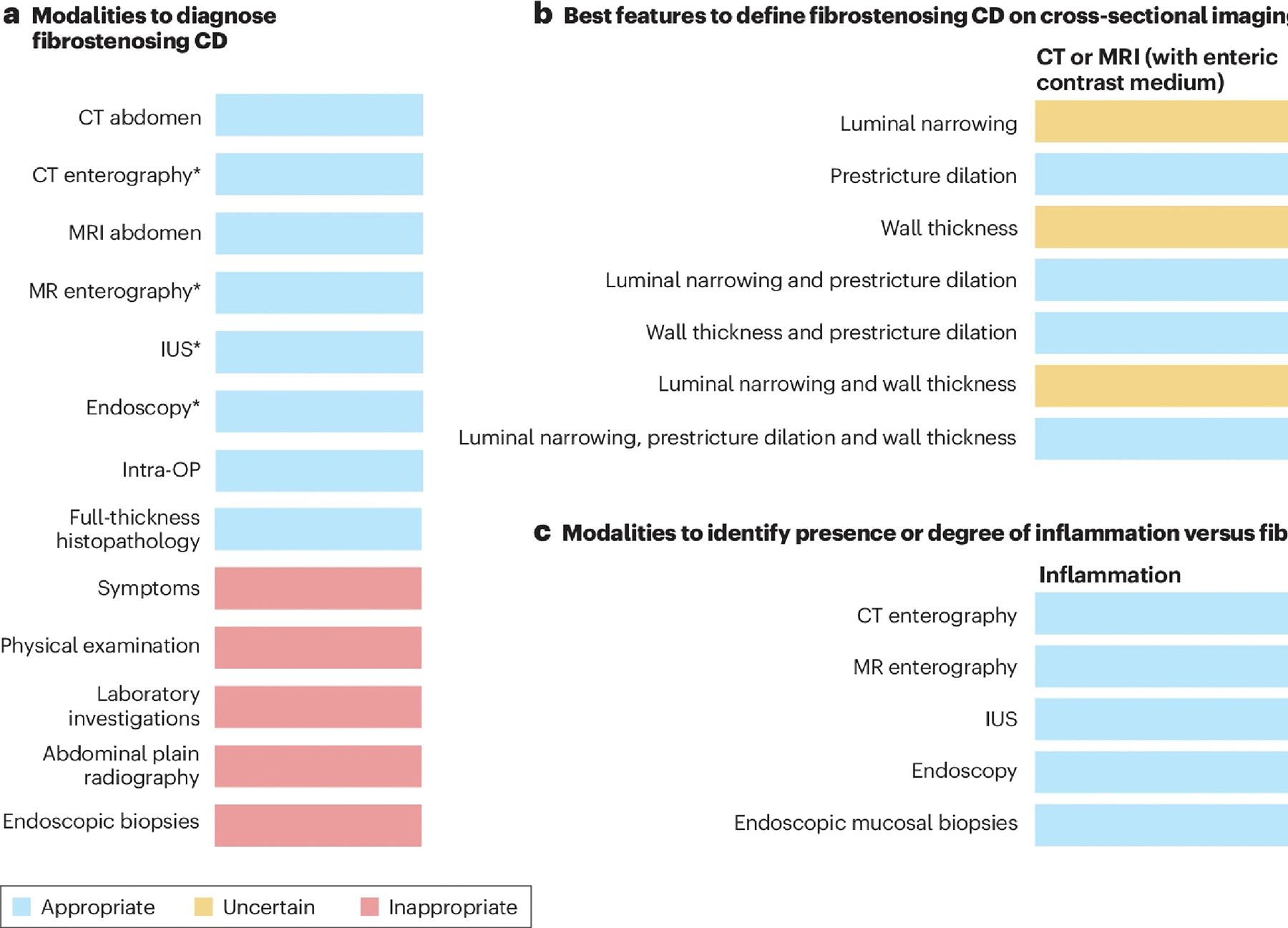
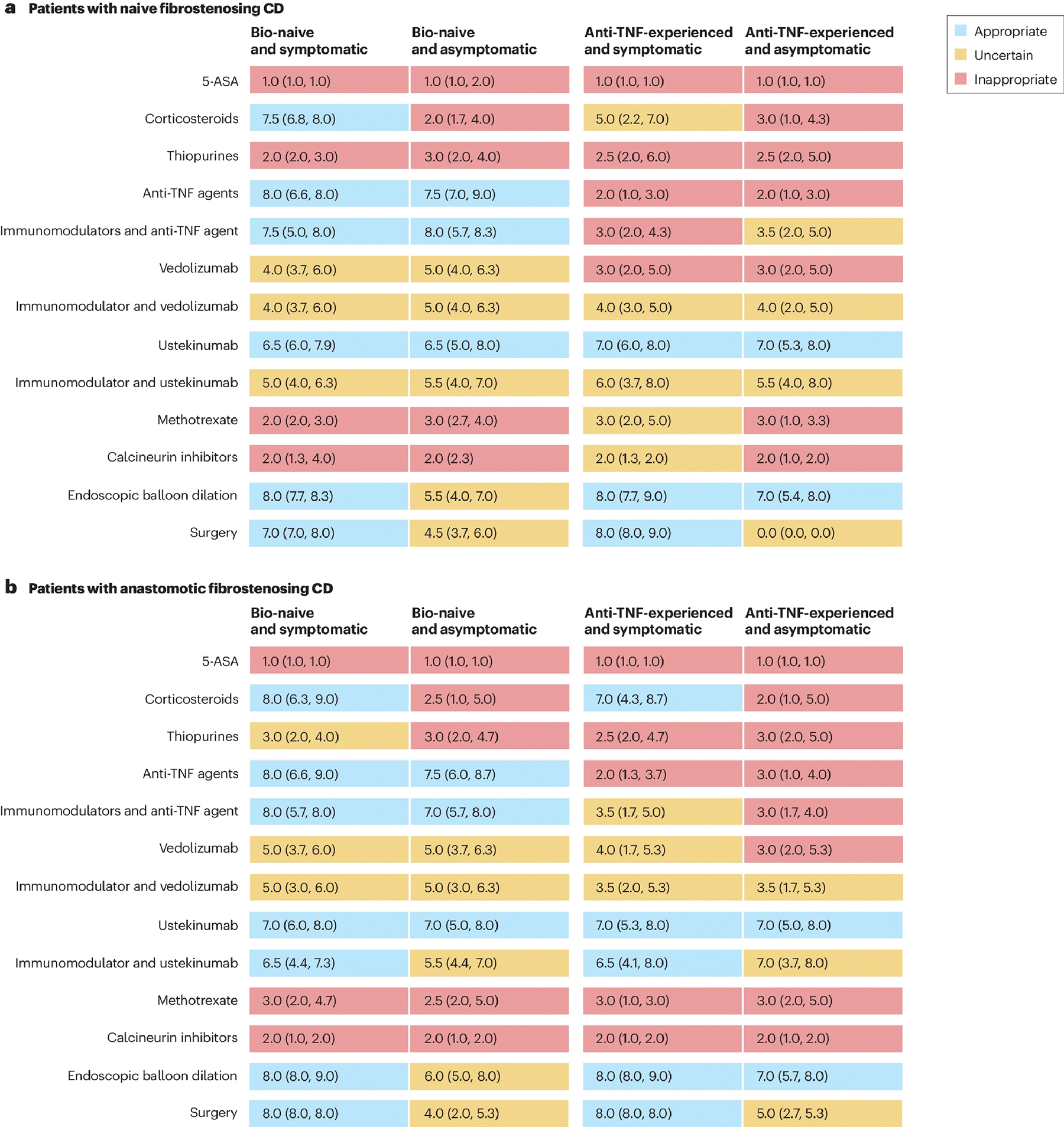
Fibrostenosis of the small bowel is common in patients with Crohn's disease. No consensus recommendations on definition, diagnosis and management in clinical practice are currently available. In this Consensus Statement, we present a clinical practice RAND/UCLA appropriateness study on the definition, diagnosis and clinical management of fibrostenosing Crohn's disease. It was conducted by a panel of 28 global experts and one patient representative. Following a systematic literature review, 526 candidate items grouped into 136 questions were generated and subsequently evaluated for appropriateness. Strictures are best defined as wall thickening, luminal narrowing and prestenotic dilation. Cross-sectional imaging is required for accurate diagnosis of fibrostenosing Crohn's disease, and it is recommended before making treatment decisions. It should also assess the degree of inflammation in the bowel wall. Multiple options for medical anti-inflammatory, endoscopic and surgical therapies were suggested, including follow-up strategies following therapy. This Consensus Statement supports clinical practice through providing guidance on definitions, diagnosis and therapeutic management of patients with fibrostenosing small bowel Crohn's disease.
© 2024. Springer Nature Limited.
Conflict of interest statement
Competing interests
D.B. is on the advisory board or consultant for AbbVie, Amgen, Arena, Atheneum, BNG Service GmbH, Bristol Myers Squibb, CED-Service GmbH, Celltrion, DGVS, Diaplan, Doctorflix, Else Kröner-Fresenius Foundation, Falk Foundation, Galapagos, Guidepoint, Impulze, Ferring, Janssen Cilag, Lilly, Medical Tribune, Med Today, MedTriX, MSD, Mylan, Onkowissen, Pharmacosmos, Pfizer, Roche, Sandoz, Takeda, Tetrameros, Thieme, Tillotts Pharma, UCB Biopharma, Viatris and Vifor Pharma. I.D. has served as a speaker, consultant and advisory board member for Takeda, Janssen, AbbVie, Pfizer, Ferring, Roche/Genentech, Celgene/BMS, Falk Pharma, Rafa Laboratories, Neopharm, Nestle, Arena, Gilead, MSD, DSM, Celltrion, Sublimity, Sandoz, Abbott and Athos Therapeutics. R.F. has served as central reader for Alimentiv, received speaker’s fees from Janssen Pharmaceuticals and consulting fee from Decibio. M.E.B. receives no direct support. Cleveland Clinic receives support for him from Siemens Healthineers in the form of salary, software and hardware for the investigation of reduced exposure in CT enterography. S.A.T. is a research consultant to Robarts. J.P. received financial support for research from AbbVie and Pfizer; consultancy fees/honorarium from AbbVie, Arena, Athos, Atomwise, Boehringer Ingelheim, Celgene, Celltrion, Ferring, Galapagos, Genentech/Roche, GlaxoSmithKline, Janssen, Mirum, Morphic, Nestlé, Origo, Pandion, Pfizer, Progenity, Protagonist, Revolo, Robarts, Takeda, Theravance and Wasserman; reports payment for lectures including service on speaker’s bureau from Abbott, Ferring, Janssen, Pfizer and Takeda; and reports payment for development of educational presentations from Abbott, Janssen, Pfizer, Roche and Takeda. J.R. is on the advisory board or consultant for Alimentiv, Boehringer Ingelheim, Janssen, Origo, Takeda and TiGenix; and received research grants from AbbVie and Genentech. W.B. served as speaker for Johnson & Johnson, Braun and Takeda; and obtained research grants from Braun, VIFOR and Medtronic. A.d’H. has served as speaker for Johnson & Johnson and Takeda. A.D. has received research support or acted as a principal investigator for AbbVie, Arena, Dr. Falk Pharma, Celgene, Gilead, Janssen and Takeda; has acted as a consultant or AbbVie, Amgen, BMS, Boehringer Ingelheim, Celgene, Dr Falk Pharma, Ferring, Fresenius Kabi, Celltrion, Janssen, Lilly, MSD, Pfizer, Pharmacosmos, Roche, Takeda, Tillotts and Vifor; and has participated in speaker’s bureaus for AbbVie, Amgen, Falk Foundation, Ferring, Janssen, Lilly, Med Today, Med Update, MSD, Pfizer, Roche, Streamed-up, Takeda, Tillotts and Vifor. W.J.S. reports consulting fees from Abbvie, Abivax, Alfasigma, Alimentiv, Beigene, Biora (Progenity), Celltrion, Forbion, Genentech, Gossamer Biosciences, Index Pharmaceuticals, Prometheus Biosciences, Protagonist Therapeutics, Shoreline Biosciences, Vedanta Biosciences, Ventyx Biosciences and Zealand Pharma; stock or stock options from BeiGene, Gossamer Bio, Biora (Progenity), Prometheus Biosciences, Prometheus Laboratories, Shoreline Biosciences, Ventyx Biosciences, Vimalan Biosciences, Vivreon Gastrosciences; and is an employee at Shoreline Biosciences and Ventyx Biosciences (spouse: Iveric Bio (consultant, stock options); Biora (Progenity) (stock); Prometheus Biosciences (employee, stock, stock options); Prometheus Laboratories (stock, stock options); Ventyx Biosciences (stock, stock options); and Vimalan Biosciences (stock)). S.C.N. served as a speaker for AbbVie, Janssen, Tillotts, Menarini, Ferring, Takeda and Pfizer; and received research funding from Olympus, Janssen and Ferring. C.L. has received consulting fees from AbbVie, Janssen, Takeda, Fresenius Kabi, Ferring, Eli Lilly; speaker’s fees from AbbVie, Janssen and Fresenius Kabi. D.H.B. is a consultant for Medtronics and Janssen; and receives research support from Medtronics and Takeda. G.R. is a consultant for Abbott, AbbVie, Augurix, Boehringer, Calypso, FALK, Ferring, Fisher, Genentech, Essex/MSD, Novartis, Pfizer, Phadia, Roche, Takeda, Tillots, UCB, Vifor, Vital Solutions and Zeller; received speaker’s honoraria from AstraZeneca, Abbott, AbbVie, FALK, MSD, Phadia, Tillots, UCB and Vifor; and received educational grants and research grants from Abbot, AbbVie, Ardeypharm, Augurix, Calypso, Essex/MSD, FALK, Flamentera, Novartis, Roche, Takeda, Tillots, UCB and Zeller. B.V. Received research support from AbbVie, Biora Therapeutics, Pfizer, Sossei Heptares and Takeda; speaker’s fees from Abbvie, Biogen, Bristol Myers Squibb, Celltrion, Chiesi, Falk, Ferring, Galapagos, Janssen, MSD, Pfizer, R-Biopharm, Takeda, Truvion and Viatris; and consultancy fees from Abbvie, Alimentiv, Applied Strategic, Atheneum, Biora Therapeutics, Bristol Myers Squibb, Galapagos, Guidepont, Mylan, Inotrem, Ipsos, Janssen, Progenity, Sandoz, Sosei Heptares, Takeda, Tillots Pharma and Viatris. G.d’H. reports consultancy activities for AbbVie, Agomab, Alimentiv, AstraZeneca, AM Pharma, AMT, Arena Pharmaceuticals, BMS, Boehringer Ingelheim, Celltrion, Eli Lilly, Exeliom Biosciences, Exo Biologics, Galapagos, Index Pharmaceuticals, Kaleido, Roche, Gilead, GlaxoSmithKline, Gossamerbio, Pfizer, Immunic, Johnson & Johnson, Origo, Polpharma, Procise Diagnostics, Prometheus Laboratories, Prometheus Biosciences, Progenit and Protagonist; speaker’s bureau for AbbVie, Arena, Galapagos, Gilead, Pfizer, BMS and Takeda; and fees for data monitoring board activities for Galapagos, AbbVie, AstraZeneca and Seres Health. B.S. has served as consultant for Abbvie, Arena, BMS, Boehringer, Celgene, Falk, Galapagos, Gilead, Janssen, Lilly, Pfizer, PredictImmune, Prometheus and Takeda; and received speaker’s fees from Abbvie, CED Service GmbH, Falk, Ferring, Galapagos, Janssen, Lilly, Novartis, Pfizer and Takeda (served as representative of the Charité). P.F. is consultant to Takeda. C.H. has served as a consultant or on advisory boards of AbbVie, Genentech, Janssen, Pfizer, Samsung Bioepis and Takeda. I.O.G. receives no direct support; Cleveland Clinic receives support for her from UCB, Celgene and Pliant Therapeutics. J.G.F. receives grants to his institution from Siemens Healthineers and Medtronic. V.J. receives salary support from the John and Susan McDonald Endowed IBD Chair at Western University, London, Ontario, Canada; consulting fees from AbbVie, Eli Lilly, GlaxoSmithKline, Arena Pharmaceuticals, Genentech, Pendopharm, Sandoz, Merck, Takeda, Janssen, Robarts Clinical Trials, Topivert and Celltrion; speaker’s fees from Takeda, Janssen, Shire, Ferring, Abbvie and Pfizer. B.G.F. has received grant and research support from Millennium Pharmaceuticals, Merck, Tillotts Pharma AG, AbbVie, Novartis Pharmaceuticals, Centocor Inc., Elan/Biogen, UCB Pharma, Bristol-Myers Squibb, Genentech, ActoGenix and Wyeth Pharmaceuticals Inc.; consulting fees from Millennium Pharmaceuticals, Merck, Centocor Inc., Elan/Biogen, Janssen-Ortho, Teva Pharmaceuticals, Bristol-Myers Squibb, Celgene, UCB Pharma, AbbVie, AstraZeneca, Serono, Genentech, Tillotts Pharma AG, Unity Pharmaceuticals, Albireo Pharma, Given Imaging Inc., Salix Pharmaceuticals, Novo Nordisk, GSK, Actogenix, Prometheus Therapeutics and Diagnostics, Athersys, Axcan, Gilead, Pfizer, Shire, Wyeth, Zealand Pharma, Zyngenia, GiCare Pharma Inc. and Sigmoid Pharma; and speaker’s bureau fees from UCB, AbbVie and J&J/Janssen. F.R. is consultant to Adnovate, Agomab, Allergan, AbbVie, Arena, Boehringer-Ingelheim, Celgene/BMS, CDISC, Celsius, Cowen, Ferring, Galapagos, Galmed, Genentech, Gilead, Gossamer, Guidepoint, Helmsley, Horizon Therapeutics, Image Analysis Limited, Index Pharma, Jannsen, Koutif, Mestag, Metacrine, Mopac, Morphic, Organovo, Origo, Pfizer, Pliant, Prometheus Biosciences, Receptos, RedX, Roche, Samsung, Surmodics, Surrozen, Takeda, Techlab, Theravance, Thetis, UCB, Ysios and 89Bio. The other authors declare no competing interests.
Figures
References
-
- Torres J, Mehandru S, Colombel JF & Peyrin-Biroulet L Crohn’s disease. Lancet 389, 1741–1755 (2017). - PubMed
-
- Farmer RG, Whelan G & Fazio VW Long-term follow-up of patients with Crohn’s disease. Relationship between the clinical pattern and prognosis. Gastroenterology 88, 1818–1825 (1985). - PubMed
-
-
Bettenworth D et al. Assessment of Crohn’s disease-associated small bowel strictures and fibrosis on cross-sectional imaging: a systematic review. Gut 68, 1115–1126 (2019).
This systematic review provides a comprehensive summary of currently used radiological approaches for detection and characterization of fibrostenosing Crohn’s disease.
-
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
