

Whole genome sequencing of HER2-positive metastatic extramammary Paget's disease: a case report
- PMID: 38831459
- PMCID: PMC11149212
- DOI: 10.1186/s13023-024-03169-y
Whole genome sequencing of HER2-positive metastatic extramammary Paget's disease: a case report
Abstract
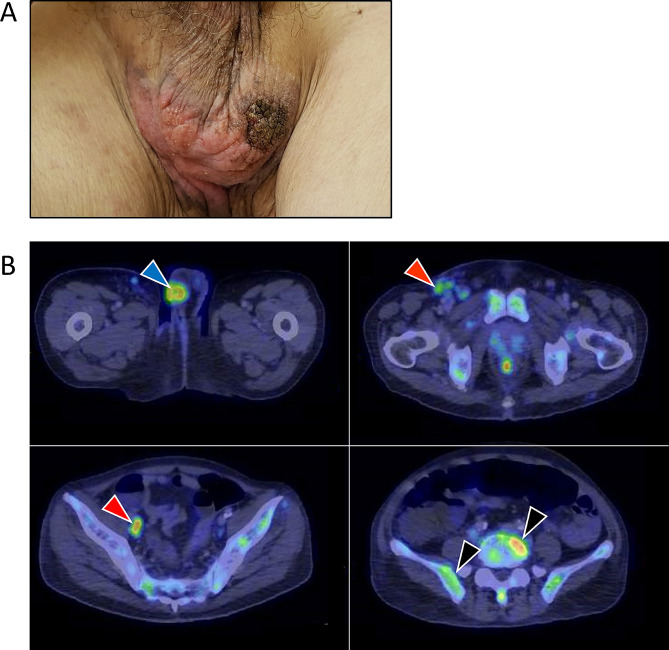
Background: Extramammary Paget's disease (EMPD) is a rare cancer that occurs within the epithelium of the skin, arising predominantly in areas with high apocrine gland concentration such as the vulva, scrotum, penis and perianal regions. Here, we aim to integrate clinicopathological data with genomic analysis of aggressive, rapidly-progressing de novo metastatic EMPD responding to HER2-directed treatment in combination with other agents, to attain a more comprehensive understanding of the disease landscape.
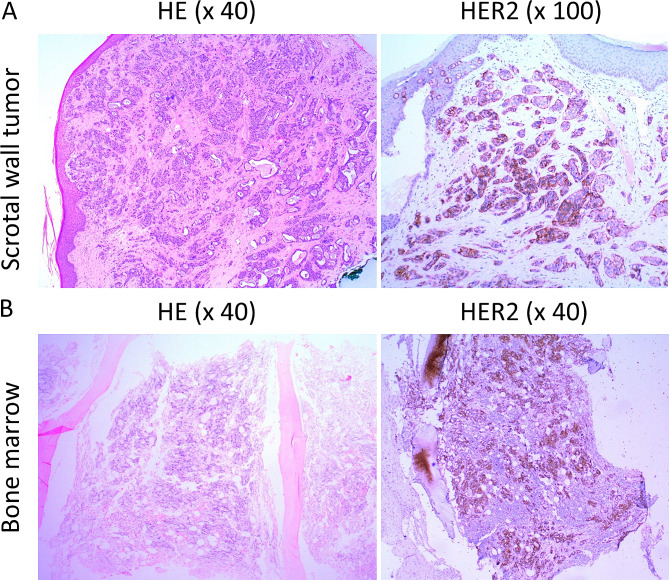
Methods: Immunohistochemical staining on the scrotal wall tumor and bone marrow metastasis demonstrated HER2 overexpression. Whole genome sequencing of the tumor and matched blood was performed.
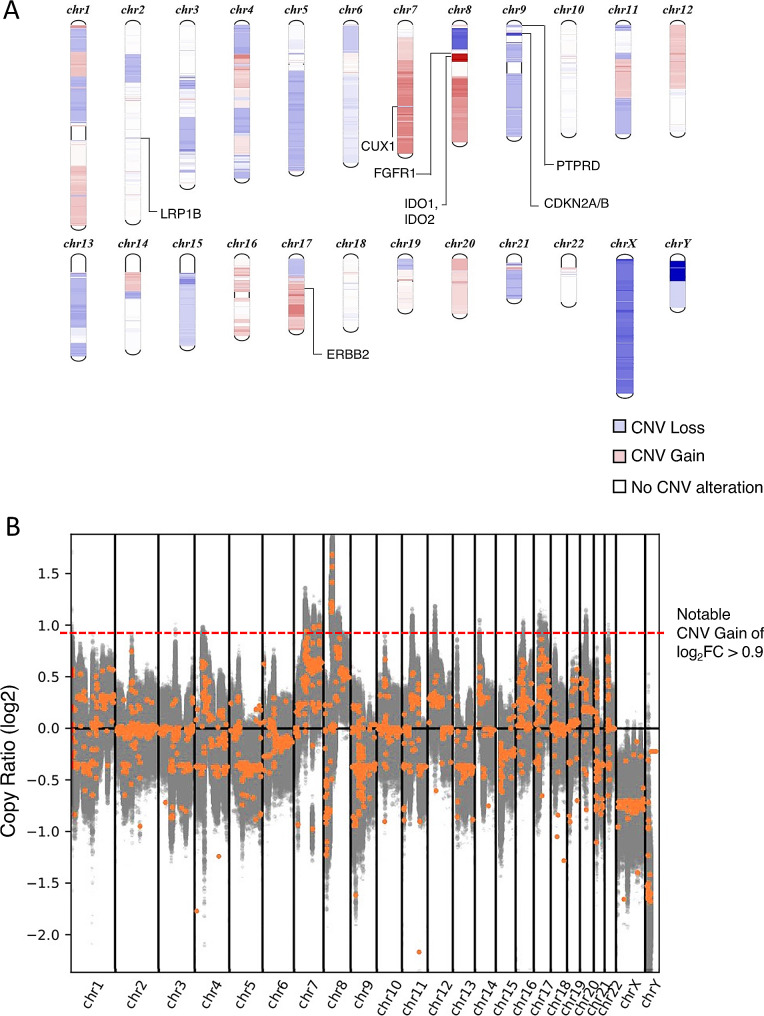
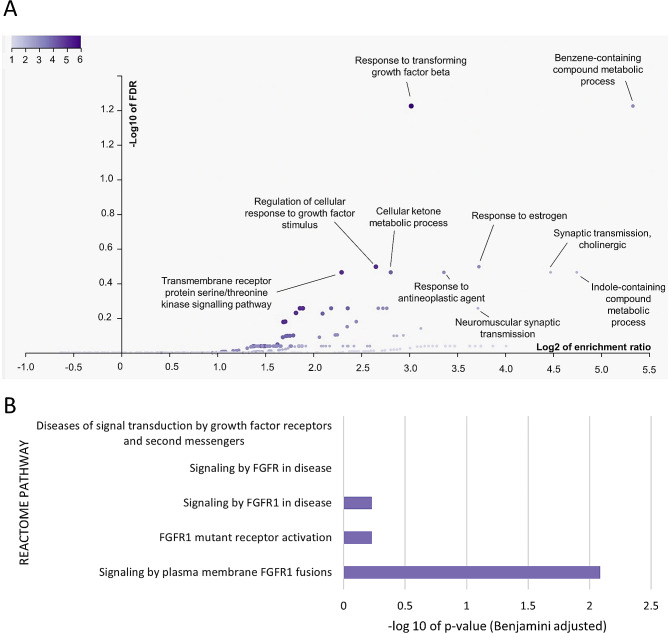
Results: Notable copy number gains (log2FC > 0.9) on chromosomes 7 and 8 were detected (n = 81), with 92.6% of these unique genes specifically located on chromosome 8. Prominent cancer-associated genes include ZNF703, HOOK3, DDHD2, LSM1, NSD3, ADAM9, BRF2, KAT6A and FGFR1. Interestingly, ERBB2 gene did not exhibit high copy number gain (log2FC = 0.4) although 90% of tumor cells stained HER2-positive. Enrichment in pathways associated with transforming growth factor-beta (TGFβ) (FDR = 0.0376, Enrichment Ratio = 8.12) and fibroblast growth factor receptor (FGFR1) signaling (FDR = 0.0082, Enrichment Ratio = 2.3) was detected. Amplicon structure analysis revealed that this was a simple-linear amplification event.
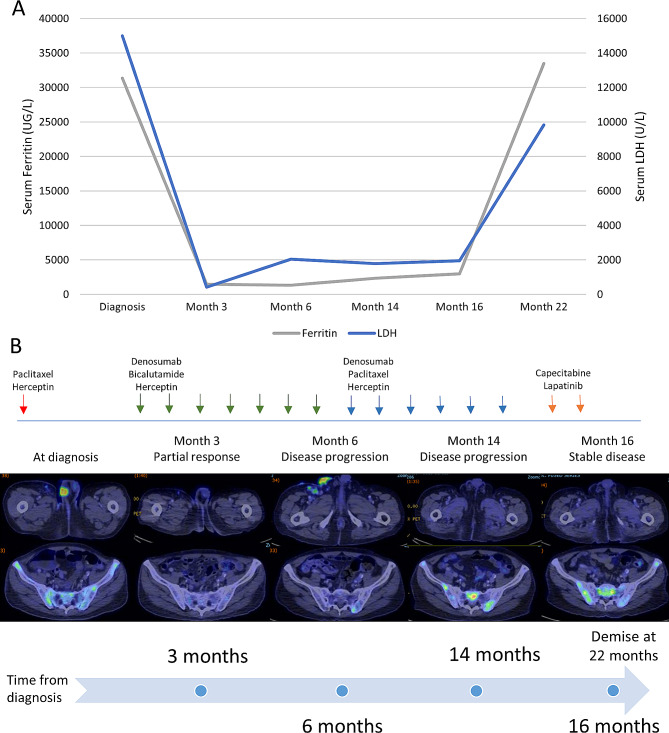
Conclusion: Whole genome sequencing revealed the underlying copy number variation landscape in HER2-positive metastatic EMPD. The presence of alternative signalling pathways and genetic variants suggests potential interactions with HER2 signalling, which possibly contributed to the HER2 overexpression and observed response to HER2-directed therapy combined with other agents in a comprehensive treatment regimen.
Keywords: ERBB2; Next generation sequencing; Precision oncology; Targeted therapy; Trastuzumab.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- St. Claire K, Hoover A, Ashack K, Khachemoune A. Extramammary Paget disease. Dermatol Online J 2019;25. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- TA21jun-0005/Singapore Ministry of Health's National Medical Research Council
- SEEDFD21jun-0002/Singapore Ministry of Health's National Medical Research Council
- CG21APR2002/Singapore Ministry of Health's National Medical Research Council
- 08/FY2023/EX/27-A65/SingHealth Duke-NUS AM/ACP-Designated Philanthropic Fund Grant Award
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
