

Efficacy and safety of long-acting injectable versus oral antipsychotics in the treatment of patients with early-phase schizophrenia-spectrum disorders: a systematic review and meta-analysis
- PMID: 38831918
- PMCID: PMC11145998
- DOI: 10.1177/20451253241257062
Efficacy and safety of long-acting injectable versus oral antipsychotics in the treatment of patients with early-phase schizophrenia-spectrum disorders: a systematic review and meta-analysis
Abstract
Background: Long-acting injectable antipsychotics (LAIs) have advantages over oral antipsychotics (OAPs) in preventing relapse and hospitalization in chronically ill patients with schizophrenia-spectrum disorders (SSDs), but evidence in patients with first-episode/recent-onset, that is, early-phase-SSDs is less clear.
Objectives: To assess the relative medium- and long-term efficacy and safety of LAIs versus OAPs in the maintenance treatment of patients with early-phase SSDs.
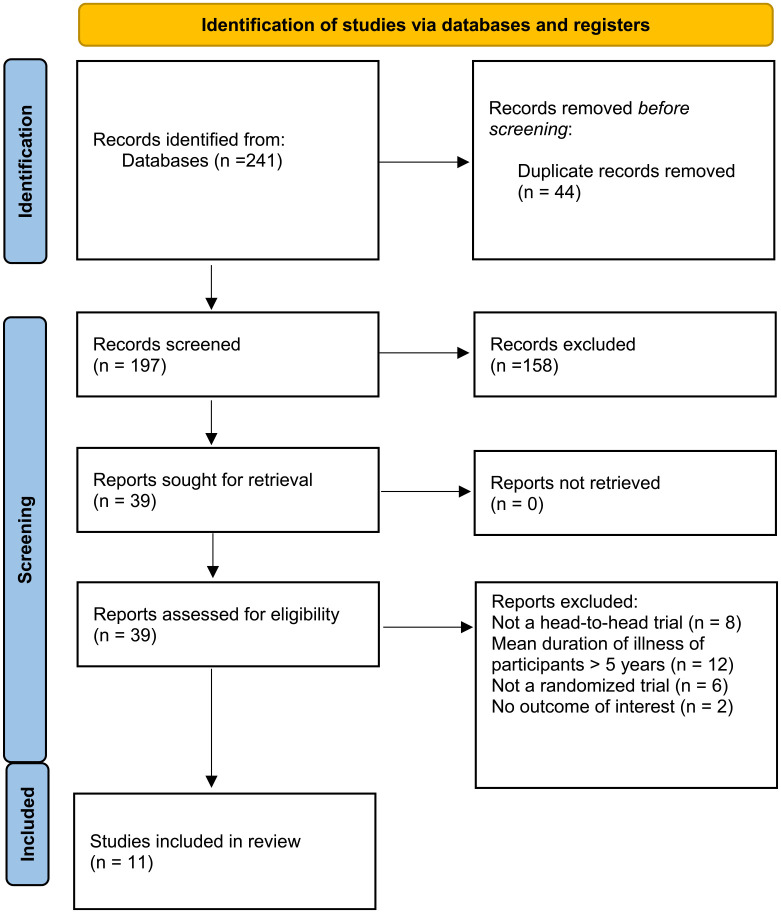
Method: We searched major electronic databases for head-to-head randomized controlled trials (RCTs) comparing LAIs and OAPs for the maintenance treatment of patients with early-phase-SSDs.
Design: Pairwise, random-effects meta-analysis. Relapse/hospitalization and acceptability (all-cause discontinuation) measured at study-endpoint were co-primary outcomes, calculating risk ratios (RRs) with their 95% confidence intervals (CIs). Subgroup analyses sought to identify factors moderating differences in efficacy or acceptability between LAIs and OAPs.
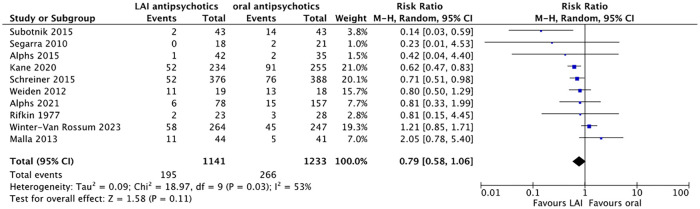
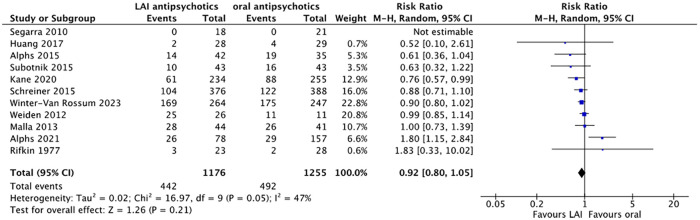
Results: Across 11 head-to-head RCTs (n = 2374, median age = 25.2 years, males = 68.4%, median illness duration = 45.8 weeks) lasting 13-104 (median = 78) weeks, no significant differences emerged between LAIs and OAPs for relapse/hospitalization prevention (RR = 0.79, 95%CI = 0.58-1.06, p = 0.13) and acceptability (RR = 0.92, 95%CI = 0.80-1.05, p = 0.20). The included trials were highly heterogeneous regarding methodology and patient populations. LAIs outperformed OAPs in preventing relapse/hospitalization in studies with stable patients (RR = 0.65, 95%CI = 0.45-0.92), pragmatic design (RR = 0.67, 95%CI = 0.54-0.82), and strict intent-to-treat approach (RR = 0.64, 95%CI = 0.52-0.80). Furthermore, LAIs were associated with better acceptability in studies with schizophrenia patients only (RR = 0.87, 95%CI = 0.79-0.95), longer illness duration (RR = 0.88, 95%CI = 0.80-0.97), unstable patients (RR = 0.89, 95%CI = 0.81-0.99) and allowed OAP supplementation of LAIs (RR = 0.90, 95%CI = 0.81-0.99).
Conclusion: LAIs and OAPs did not differ significantly regarding relapse prevention/hospitalization and acceptability. However, in nine subgroup analyses, LAIs were superior to OAPs in patients with EP-SSDs with indicators of higher quality and/or pragmatic design regarding relapse/hospitalization prevention (four subgroup analyses) and/or reduced all-cause discontinuation (five subgroup analyses), without any instance of OAP superiority versus LAIs. More high-quality pragmatic trials comparing LAIs with OAPs in EP-SSDs are needed.
Trial registration: CRD42023407120 (PROSPERO).
Keywords: early-phase psychosis; long-acting injectable antipsychotics; oral antipsychotics; schizophrenia.
Plain language summary
Comparing long-acting injections and pills for early schizophrenia: a study review and combined analysis Background: We explored whether antipsychotics long-acting injections (LAIs) might outperform regular antipsychotics pills for people dealing with early-stage conditions like schizophrenia. While LAIs have clear benefits for those with long-term challenges, their effectiveness for those just starting to grapple with these issues is less certain.
Objective: We aimed to uncover whether LAIs or regular antipsychotic pills demonstrate better outcomes over the medium and long term for individuals in the early stages of schizophrenia.
Method: We scrutinized several studies comparing LAIs to regular pills in treating early-stage schizophrenia. Employing a combined analysis, we assessed factors such as preventing relapses and hospitalizations, as well as patient treatment adherence.
Design: We combined different study results in one unique analysis. We delved into whether LAIs surpassed regular pills in preventing relapses and hospitalizations and in patient treatment adherence.
Results: In our study of 11 trials involving over 2000 participants, we observed that LAIs and regular antipsychotic pills were generally comparable regarding preventing relapses, hospitalizations, and treatment adherence. However, on closer inspection, LAIs appeared slightly more effective for specific groups in the early stages of schizophrenia.
Conclusion: While LAIs and regular antipsychotic pills showed similar results for most individuals in the early stages of schizophrenia, our findings hint at the possibility that LAIs might have a slight edge for certain groups. Nevertheless, we emphasize the need for more high-quality studies to gain a clearer understanding.
Registration: This study is registered under CRD42023407120 (PROSPERO).
© The Author(s), 2024.
Figures
References
-
- James SL, Abate D, Abate KH, et al.. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018; 392: 1789–1858. - PMC - PubMed
-
- Solmi M, Seitidis G, Mavridis D, et al.. Incidence, prevalence, and global burden of schizophrenia - data, with critical appraisal, from the global burden of disease (GBD) 2019. Mol Psychiatry 2023; 28: 5319–5327. - PubMed
-
- Perkins DO, Gu H, Weiden PJ, et al.. Predictors of treatment discontinuation and medication nonadherence in patients recovering from a first episode of schizophrenia, schizophreniform disorder, or schizoaffective disorder. J Clin Psychiatry 2008; 69: 106–113. - PubMed
LinkOut - more resources
Full Text Sources
