

Expertise in surgical neuro-oncology. Results of a survey by the EANS neuro-oncology section
- PMID: 38831935
- PMCID: PMC11145419
- DOI: 10.1016/j.bas.2024.102822
Expertise in surgical neuro-oncology. Results of a survey by the EANS neuro-oncology section
Abstract
Introduction: Technical advances and the increasing role of interdisciplinary decision-making may warrant formal definitions of expertise in surgical neuro-oncology.
Research question: The EANS Neuro-oncology Section felt that a survey detailing the European neurosurgical perspective on the concept of expertise in surgical neuro-oncology might be helpful.
Material and methods: The EANS Neuro-oncology Section panel developed an online survey asking questions regarding criteria for expertise in neuro-oncological surgery and sent it to all individual EANS members.
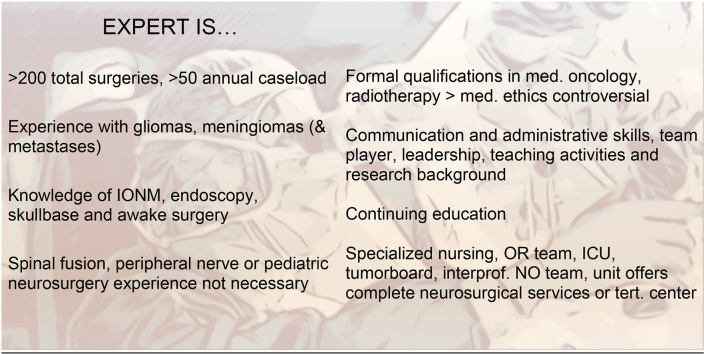
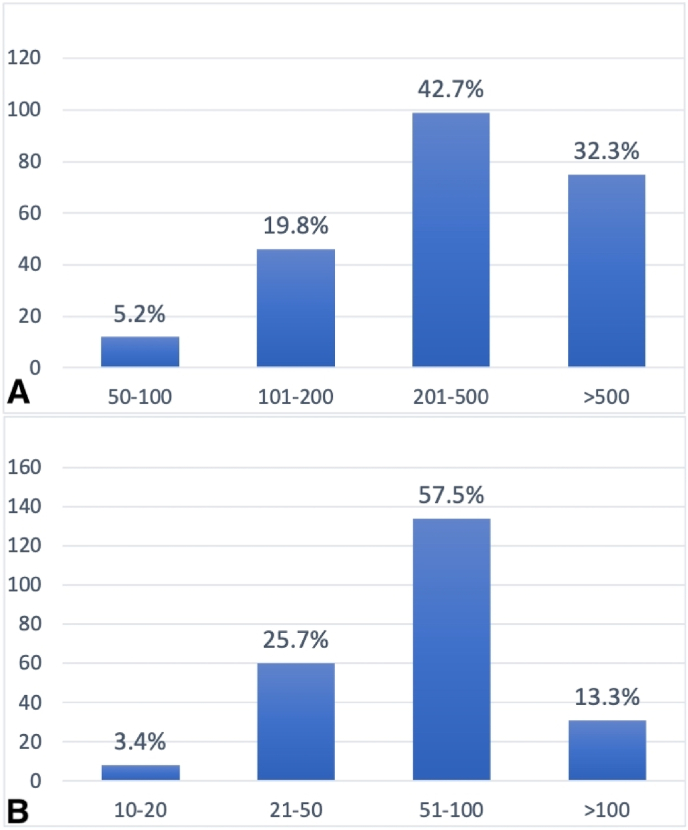
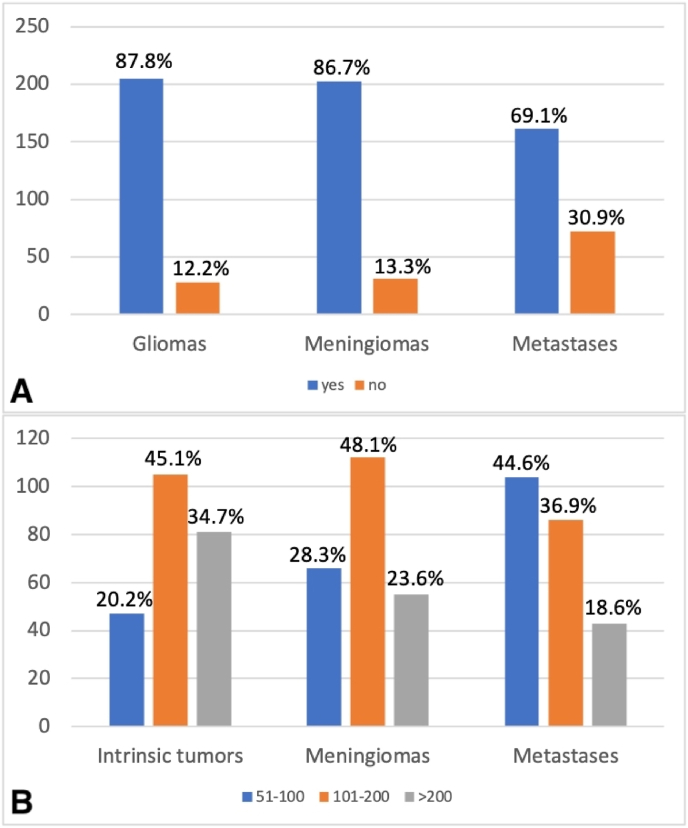
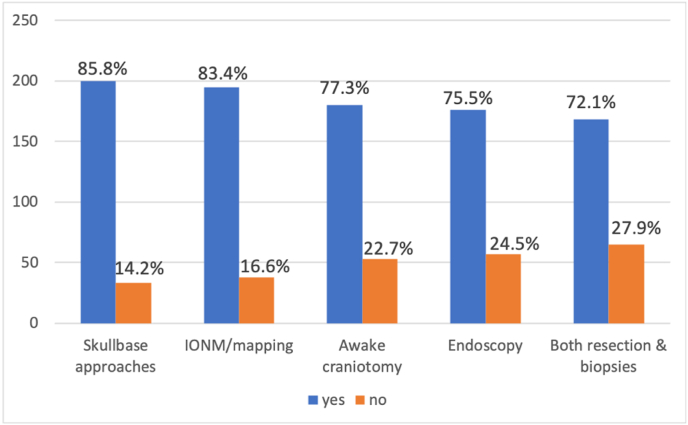
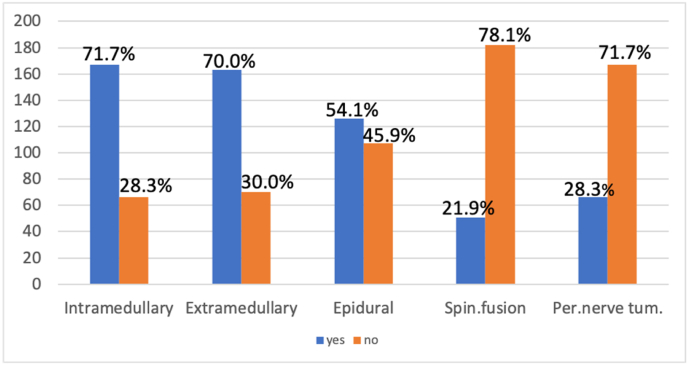
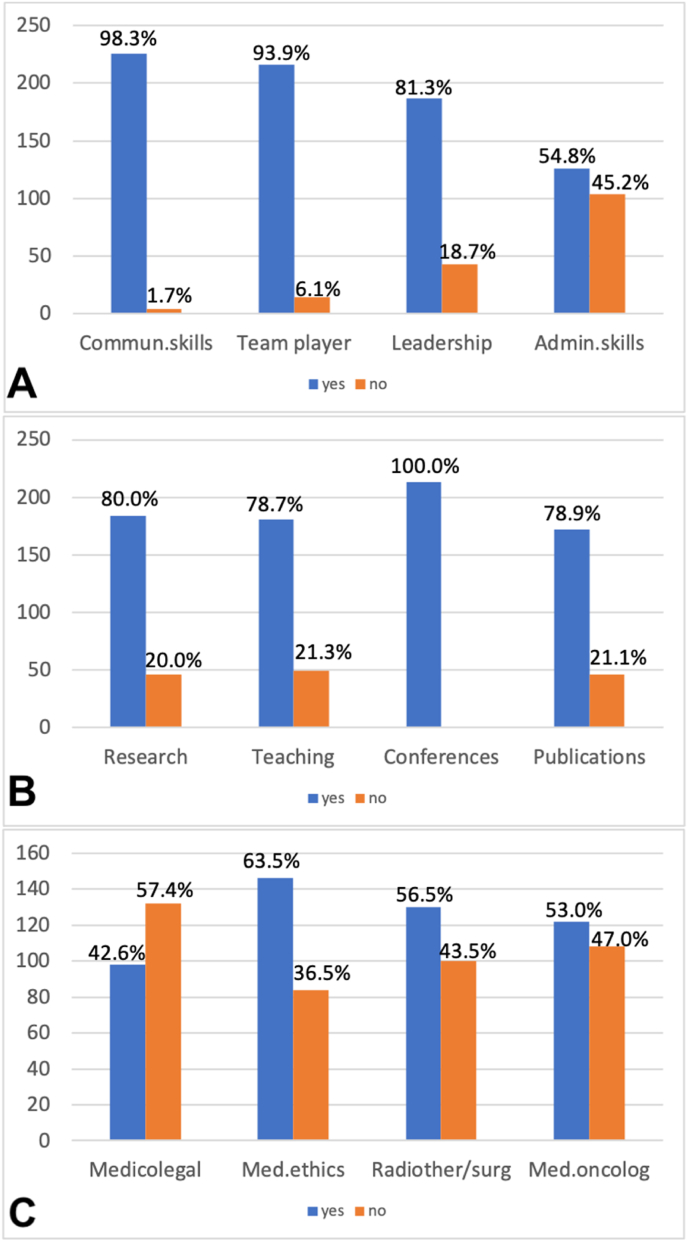
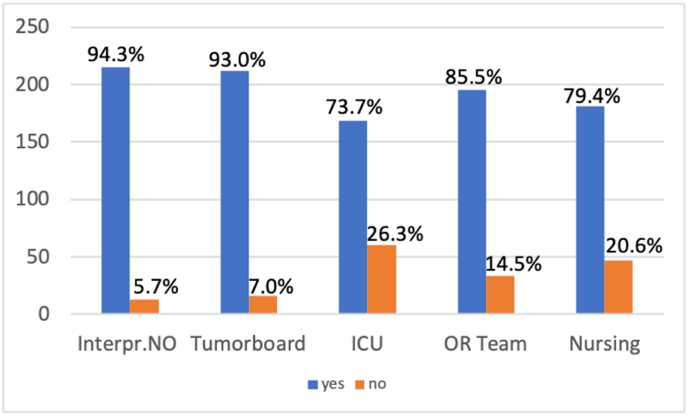
Results: Our questionnaire was completed by 251 respondents (consultants: 80.1%) from 42 countries. 67.7% would accept a lifetime caseload of >200 cases and 86.7% an annual caseload of >50 as evidence of neuro-oncological surgical expertise. A majority felt that surgeons who do not treat children (56.2%), do not have experience with spinal fusion (78.1%) or peripheral nerve tumors (71.7%) may still be considered experts. Majorities believed that expertise requires the use of skull-base approaches (85.8%), intraoperative monitoring (83.4%), awake craniotomies (77.3%), and neuro-endoscopy (75.5%) as well as continuing education of at least 1/year (100.0%), a research background (80.0%) and teaching activities (78.7%), and formal interdisciplinary collaborations (e.g., tumor board: 93.0%). Academic vs. non-academic affiliation, career position, years of neurosurgical experience, country of practice, and primary clinical interest had a minor influence on the respondents' opinions.
Discussion and conclusion: Opinions among neurosurgeons regarding the characteristics and features of expertise in neuro-oncology vary surprisingly little. Large majorities favoring certain thresholds and qualitative criteria suggest a consensus definition might be possible.
Keywords: CNS tumors; EANS; Expertise; Surgical neuro-oncology.
© 2024 Published by Elsevier B.V. on behalf of EUROSPINE, the Spine Society of Europe, EANS, the European Association of Neurosurgical Societies.
Figures
References
-
- Behling F., Bruneau M., Honegger J., Berhouma M., Jouanneau E., Cavallo L., Cornelius J.F., Messerer M., Daniel R.T., Froelich S., Mazzatenta D., Meling T., Paraskevopoulos D., Roche P.H., Schroeder H.W.S., Zazpe I., Voormolen E., Visocchi M., Kasper E., Schittenhelm J., Tatagiba M. Differences in intraoperative sampling during meningioma surgery regarding CNS invasion - results of a survey on behalf of the EANS skull base section. Brain Spine. 2023;3 - PMC - PubMed
-
- Bonrath E.M., Dedy N.J., Gordon L.E., Grantcharov T.P. Comprehensive surgical Coaching Enhances surgical skill in the operating room: a Randomized Controlled trial. Ann. Surg. 2015;262:205–212. - PubMed
-
- Carnduff M., Place R. The relation of surgical volume to competence: when is Enough, Enough? Mil. Med. 2022;187:64–67. - PubMed
-
- Dunphy B.C., Williamson S.L. In pursuit of expertise. Toward an educational model for expertise development. Adv Health Sci Educ Theory Pract. 2004;9:107–127. - PubMed
