

Collateral effects of the COVID-19 pandemic on endocrine treatments for breast and prostate cancer in the UK: a cohort study
- PMID: 38832300
- PMCID: PMC11146008
- DOI: 10.1177/17588359241253115
Collateral effects of the COVID-19 pandemic on endocrine treatments for breast and prostate cancer in the UK: a cohort study
Abstract
Background: The COVID-19 pandemic affected cancer screening, diagnosis and treatments. Many surgeries were substituted with bridging therapies during the initial lockdown, yet consideration of treatment side effects and their management was not a priority.
Objectives: To examine how the changing social restrictions imposed by the pandemic affected incidence and trends of endocrine treatment prescriptions in newly diagnosed (incident) breast and prostate cancer patients and, secondarily, endocrine treatment-related outcomes (including bisphosphonate prescriptions, osteopenia and osteoporosis), in UK clinical practice from March 2020 to June 2022.
Design: Population-based cohort study using UK primary care Clinical Practice Research Datalink GOLD database.
Methods: There were 13,701 newly diagnosed breast cancer patients and 12,221 prostate cancer patients with ⩾1-year data availability since diagnosis between January 2017 and June 2022. Incidence rates (IR) and incidence rate ratios (IRR) were calculated across multiple time periods before and after lockdown to examine the impact of changing social restrictions on endocrine treatments and treatment-related outcomes, including osteopenia, osteoporosis and bisphosphonate prescriptions.
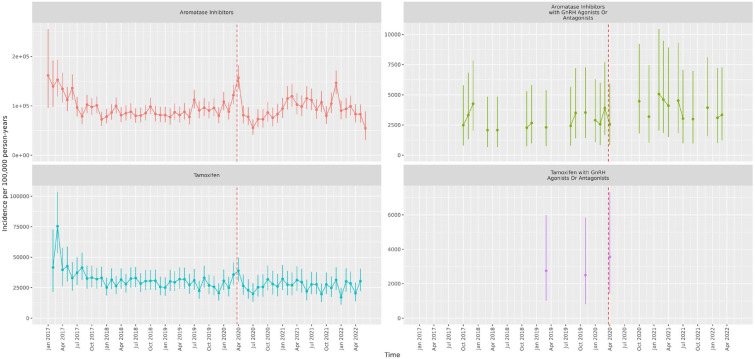
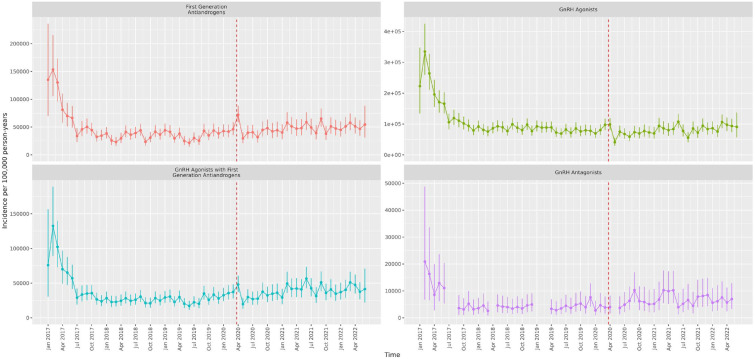
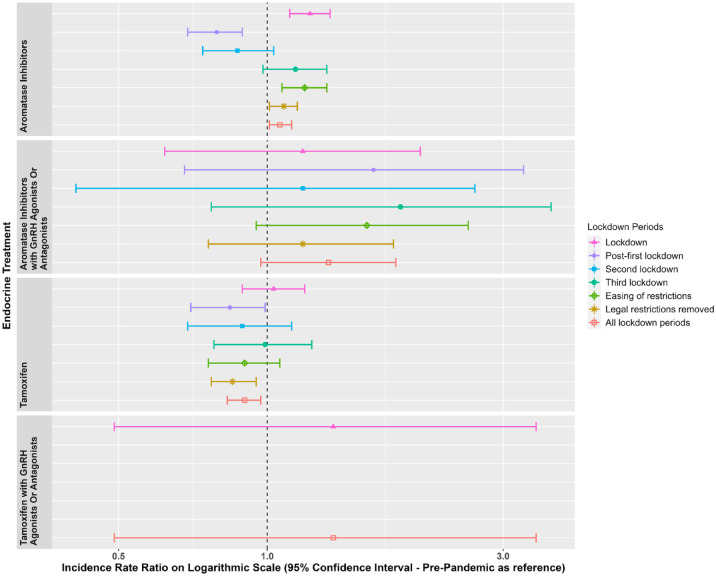
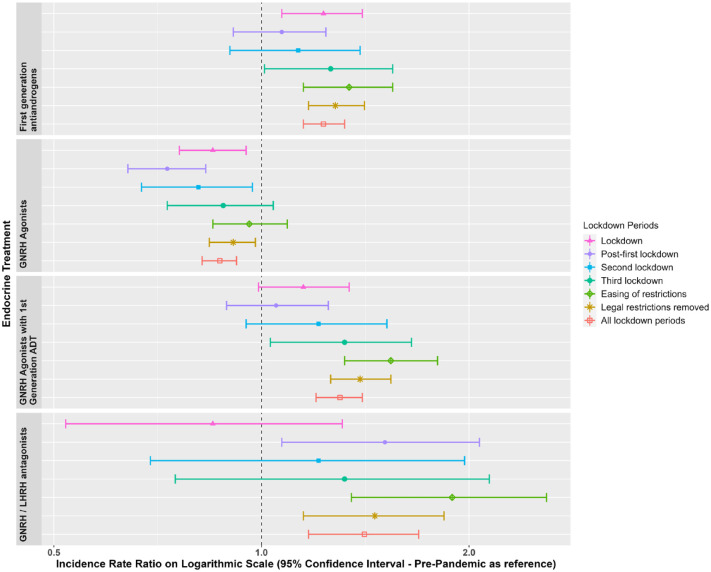
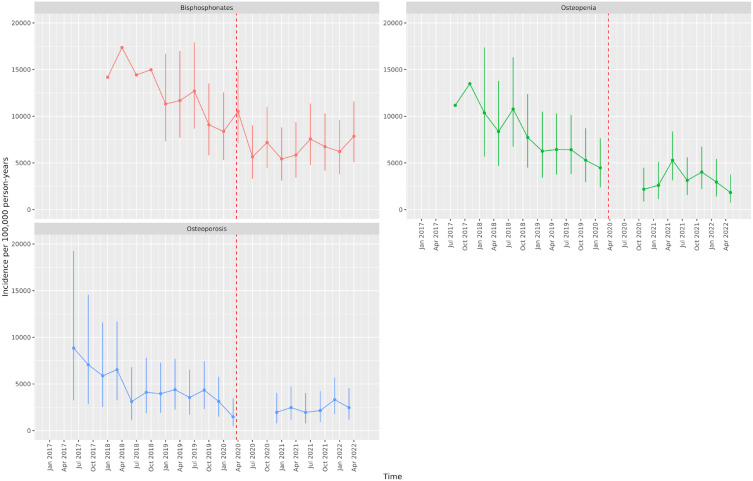
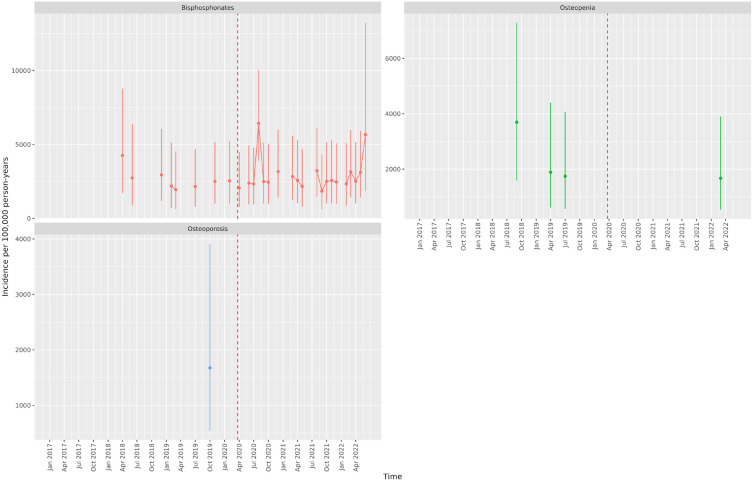
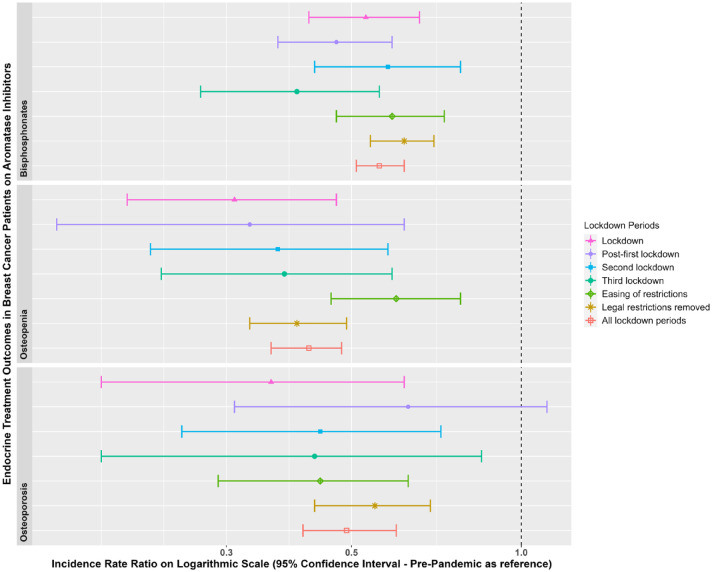
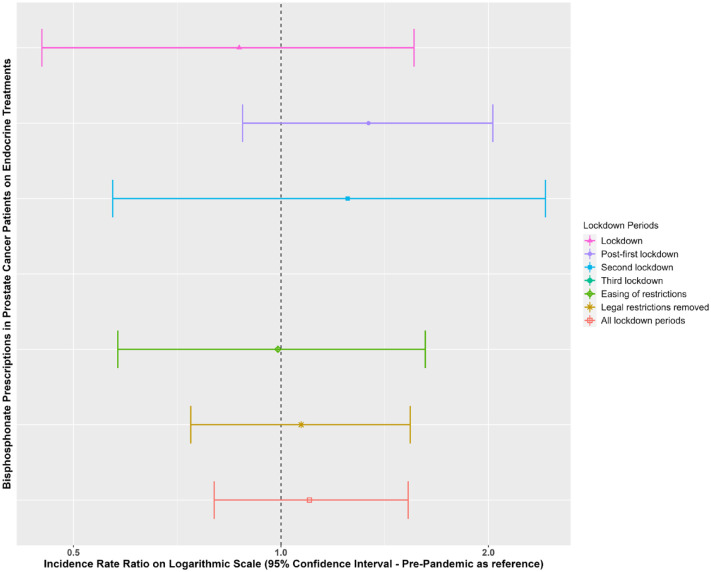
Results: In breast cancer patients, aromatase inhibitor (AI) prescriptions increased during lockdown versus pre-pandemic [IRR: 1.22 (95% confidence interval (CI): 1.11-1.34)], followed by a decrease post-first lockdown [IRR: 0.79 (95% CI: 0.69-0.89)]. In prostate cancer patients, first-generation antiandrogen prescriptions increased versus pre-pandemic [IRR: 1.23 (95% CI: 1.08-1.4)]. For breast cancer patients on AIs, diagnoses of osteopenia, osteoporosis and bisphosphonate prescriptions were reduced across all lockdown periods versus pre-pandemic (IRR range: 0.31-0.62).
Conclusion: During the first 2 years of the pandemic, newly diagnosed breast and prostate cancer patients were prescribed more endocrine treatments compared to pre-pandemic due to restrictions on hospital procedures replacing surgeries with bridging therapies. But breast cancer patients had fewer diagnoses of osteopenia and osteoporosis and bisphosphonate prescriptions. These patients should be followed up in the coming years for signs of bone thinning. Evidence of poorer management of treatment-related side effects will help assess resource allocation for patients at high risk for bone-related complications.
Keywords: COVID-19; adjuvent therapy; breast cancer; endocrine therapy < hormone therapy; pandemic; prostate cancer.
Plain language summary
Effects of the COVID-19 pandemic on hormone treatments for breast and prostate cancer in the UK: implications for bone health The COVID-19 pandemic has had a big impact on health, going beyond just causing illness. One area it has influenced is how patients with breast cancer or prostate cancer are treated. Surgeries and radiotherapies were delayed from the first lockdown as hospitals reduced non-covid related procedures. Some patients with breast or prostate cancer were instead given some medications to help stop their cancers from growing until they were able to have surgery or radiotherapy. These medications (called endocrine treatments) have important side effects, such as conditions that affect the bones. Patients on these medications should be monitored by doctors for signs of bone thinning and should, in some cases, be given other medications to help stop this happening. This study used doctors’ records from more than 5 million people to find out whether the pandemic affected the number of endocrine medications being prescribed in patients with breast or prostate cancer, and also looked at the number of these patients that were diagnosed with conditions that affect their bones and whether they were given medications that could protect their bone health. We found that during the first lockdown, patients with breast cancer or prostate cancer had more of some types of endocrine treatments compared to before the lockdown. However, they had fewer diagnoses of conditions related to bone health and fewer medications to protect their bones. It is possible that appointments and tests that are usually carried out to diagnose conditions relating to bone health were not performed in the months after the first lockdown, and so these conditions were underdiagnosed. The use of medications to protect their bones was also reduced, likely because this was not considered a priority during the pandemic. This highlights that such patients should be followed up in the coming years for signs of bone thinning, given the relatively poorer management of these side effects in these people after the pandemic.
© The Author(s), 2024.
Conflict of interest statement
DP-A’s research group has received research grants from the European Medicines Agency, the Innovative Medicines Initiative, Amgen, Chiesi and UCB Biopharma and consultancy or speaker fees from Astellas, Amgen and UCB Biopharma. DP-A receives funding from the UK National Institute for Health Research (NIHR) in the form of a senior research fellowship and the Oxford NIHR Biomedical Research Centre.
Figures
References
-
- Barclay NL, Burkard T, Burn E, et al. The impact of the COVID-19 pandemic on short-term cancer survival in the United Kingdom: a cohort analysis. MedRXiv, 2023. DOI: 10.1101/2023.09.14.23295563. - DOI
-
- Barclay NL, Pineda-Moncusí M, Jödicke AM, et al. The impact of the UK COVID-19 lockdown on the screening, diagnostics and incidence of breast, colorectal, lung and prostate cancer in the UK: a population-based cohort study. Frontiers in Oncology, 14, 2024. DOI: 10.3389/fonc.2024.1370862. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
