

Immunostimulatory CKb11 gene combined with immune checkpoint PD-1/PD-L1 blockade activates immune response and simultaneously overcomes the immunosuppression of cancer
- PMID: 38832303
- PMCID: PMC11145080
- DOI: 10.1016/j.bioactmat.2024.05.014
Immunostimulatory CKb11 gene combined with immune checkpoint PD-1/PD-L1 blockade activates immune response and simultaneously overcomes the immunosuppression of cancer
Abstract
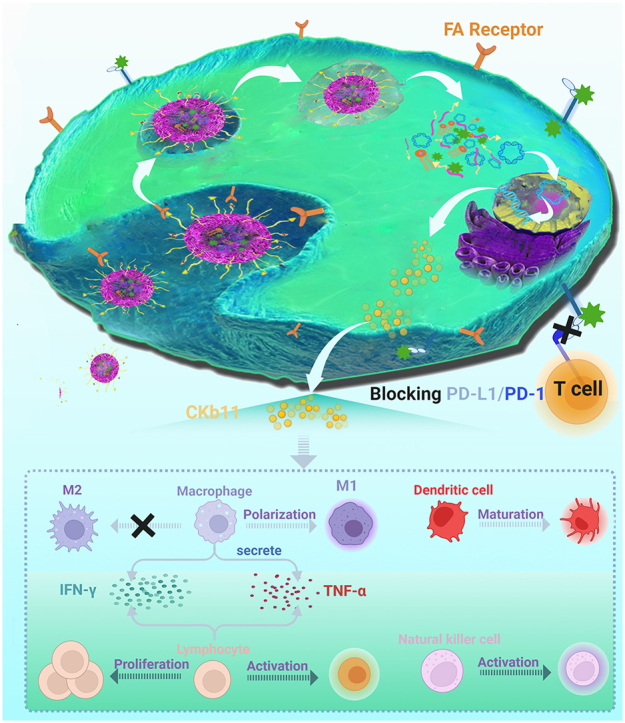
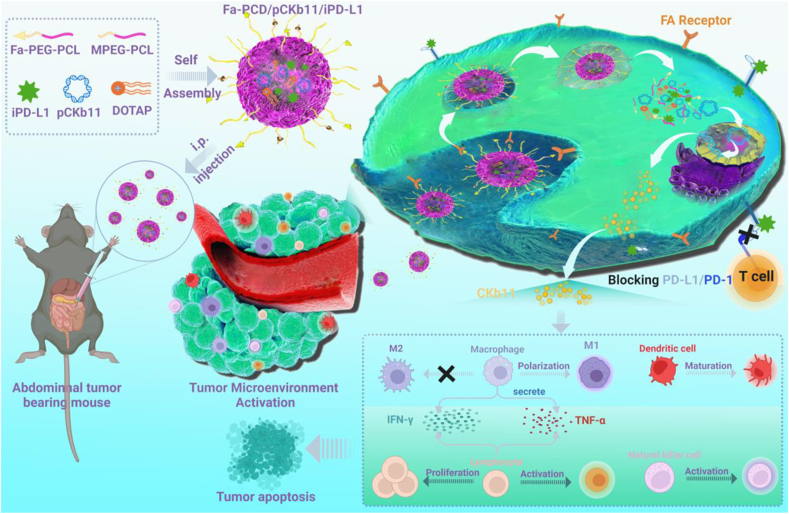
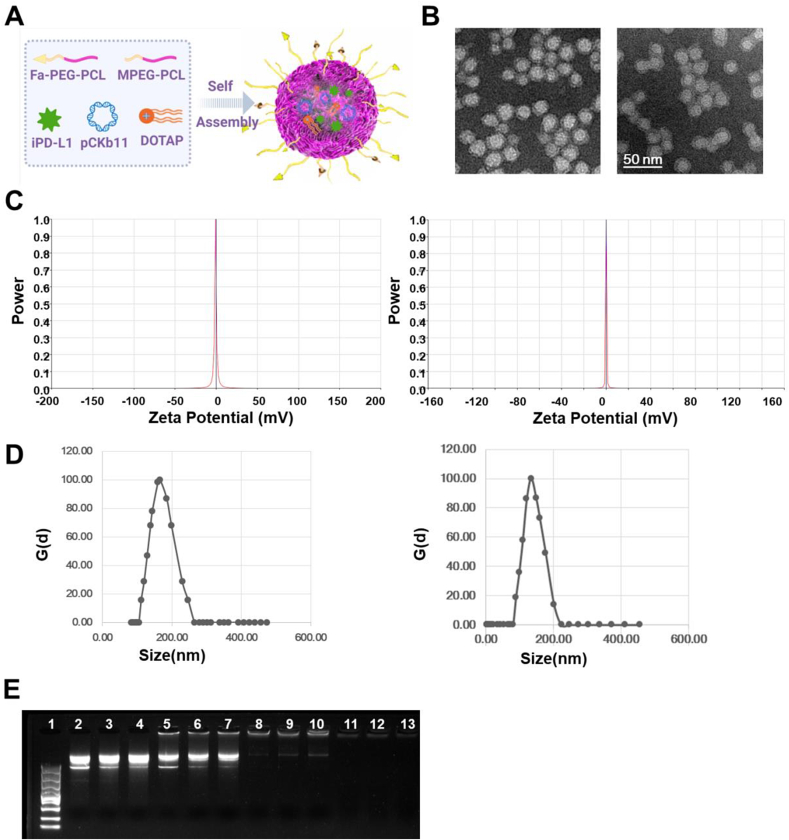
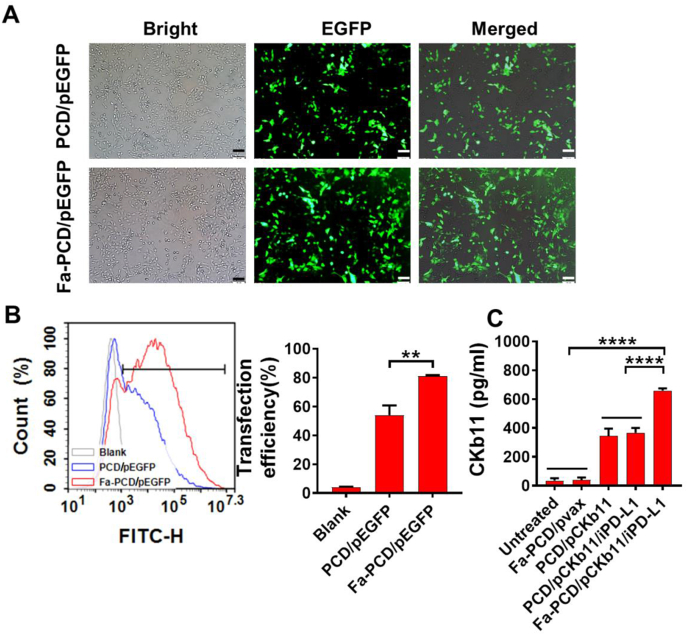
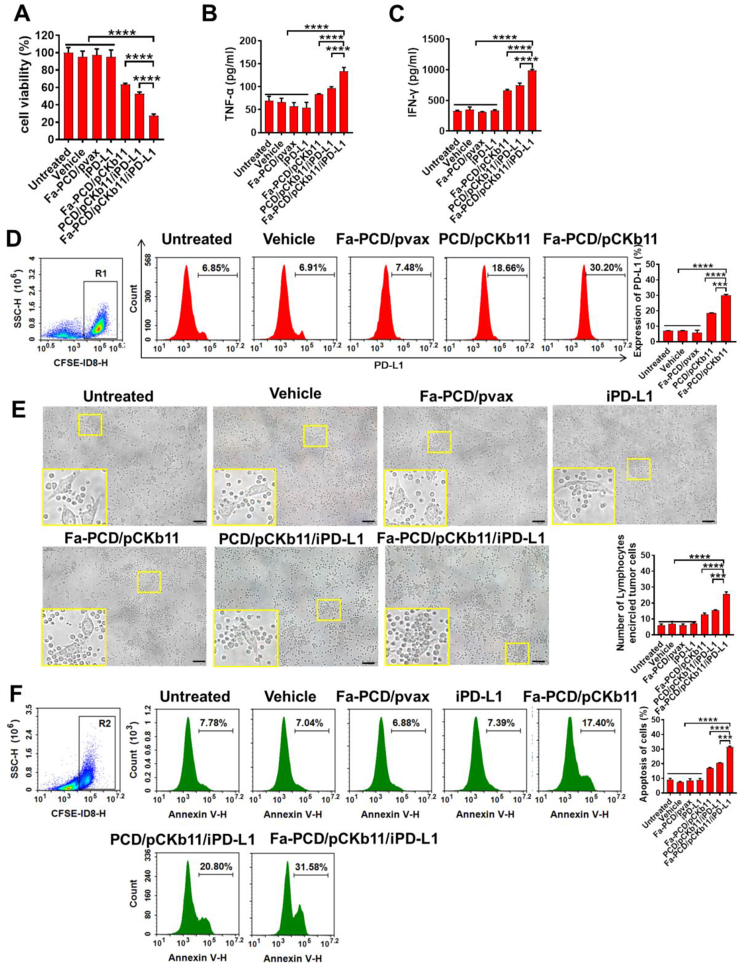
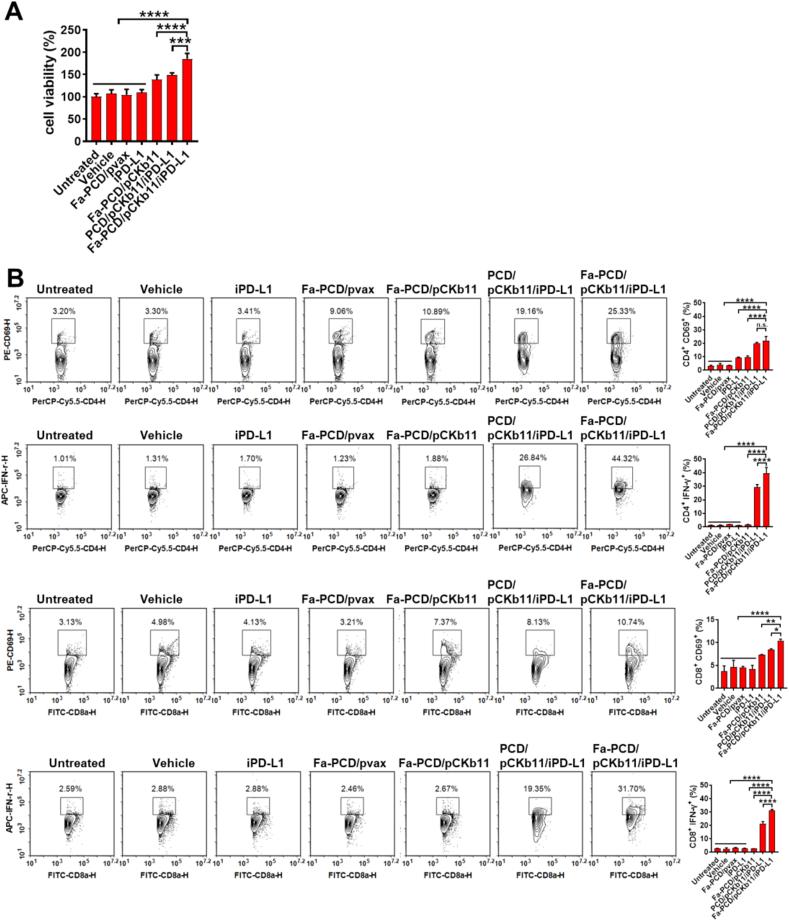
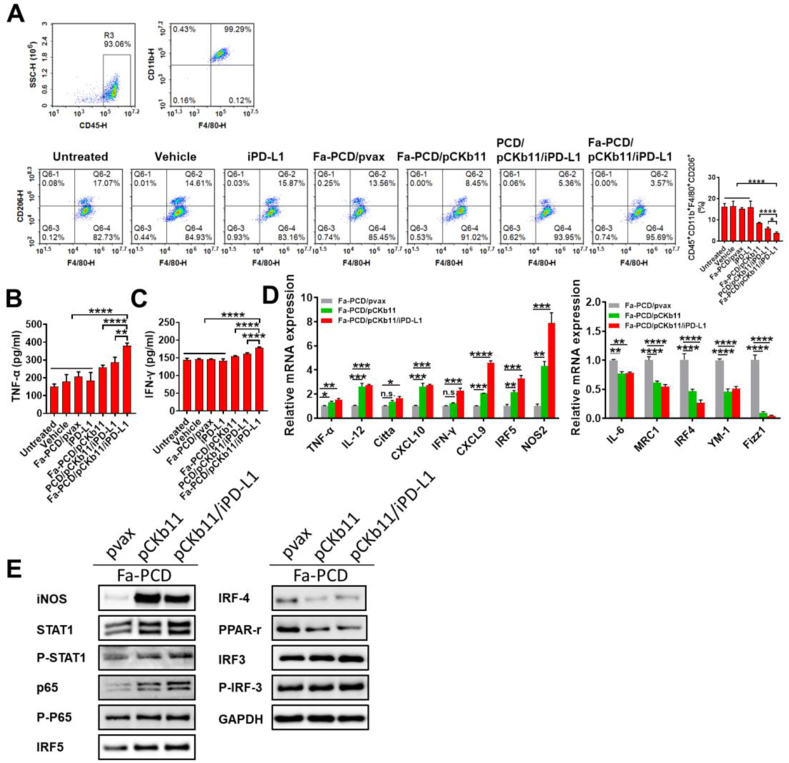
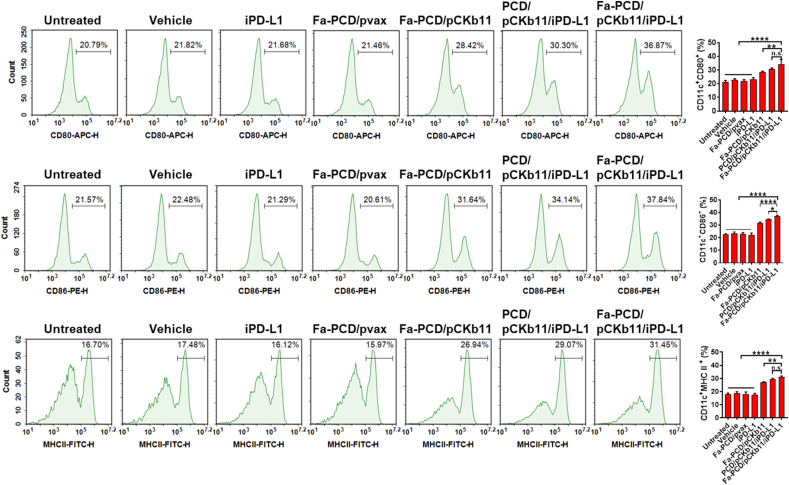
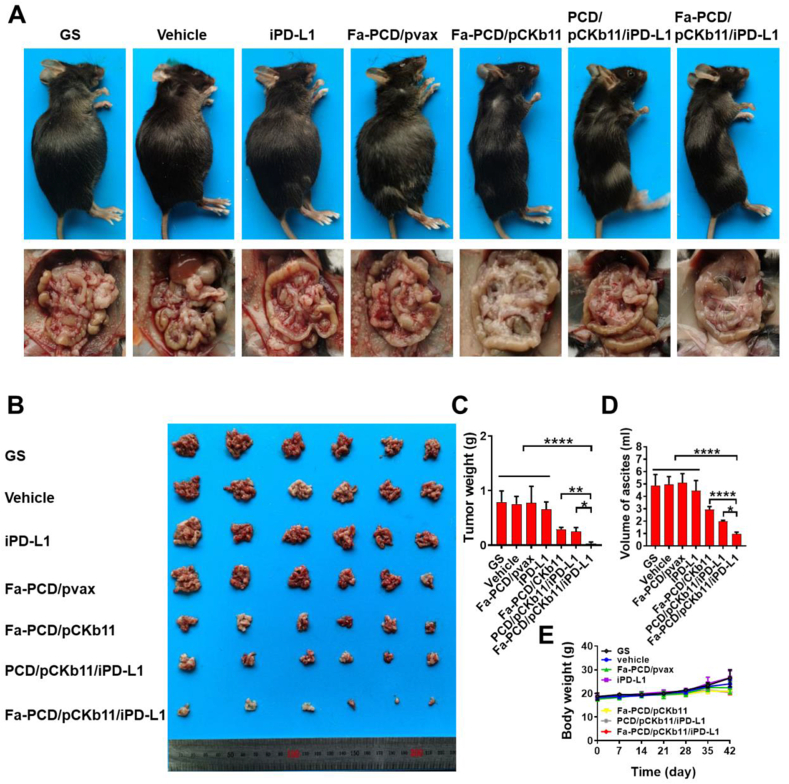
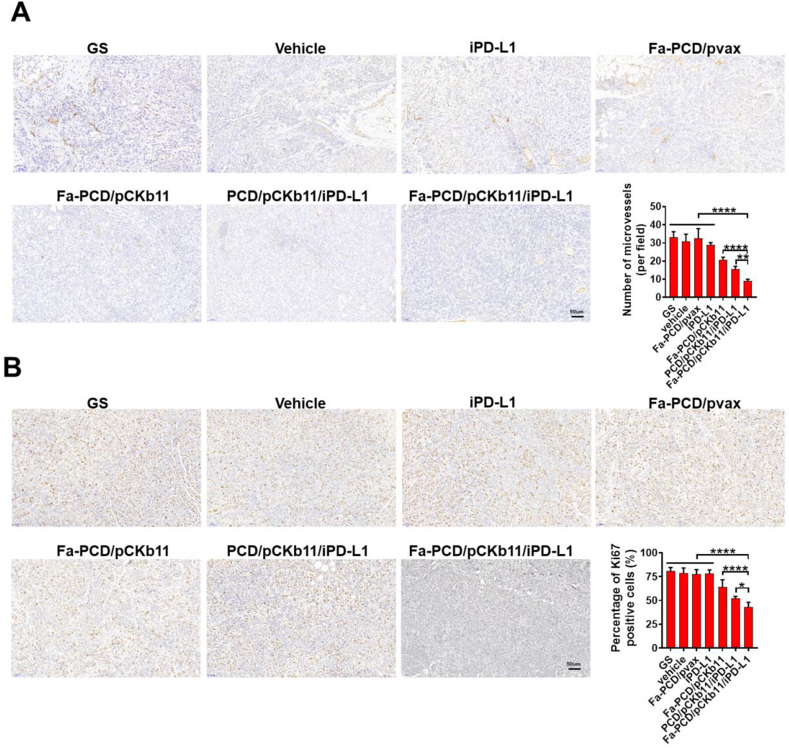
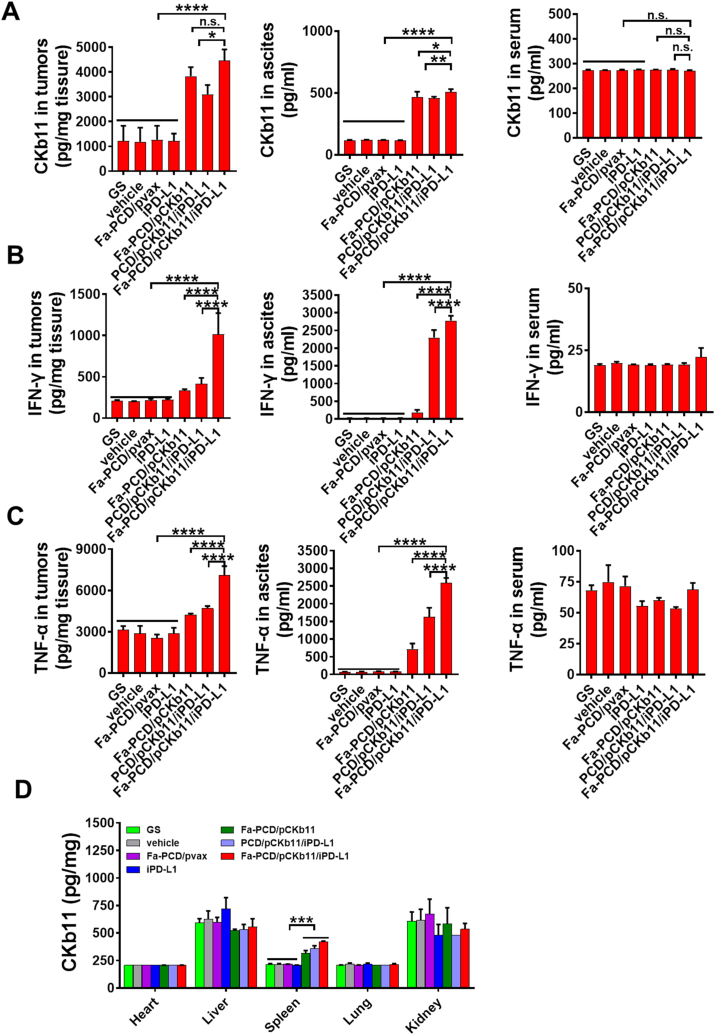
Immunosuppression tumor microenvironment (TME) seriously impedes anti-tumor immune response, resulting in poor immunotherapy effect of cancer. This study develops a folate-modified delivery system to transport the plasmids encoding immune stimulatory chemokine CKb11 and PD-L1 inhibitors to tumor cells, resulting in high CKb11 secretion from tumor cells, successfully activating immune cells and increasing cytokine secretion to reshape the TME, and ultimately delaying tumor progression. The chemokine CKb11 enhances the effectiveness of tumor immunotherapy by increasing the infiltration of immune cells in TME. It can cause high expression of IFN-γ, which is a double-edged sword that inhibits tumor growth while causing an increase in the expression of PD-L1 on tumor cells. Therefore, combining CKb11 with PD-L1 inhibitors can counterbalance the suppressive impact of PD-L1 on anti-cancer defense, leading to a collaborative anti-tumor outcome. Thus, utilizing nanotechnology to achieve targeted delivery of immune stimulatory chemokines and immune checkpoint inhibitors to tumor sites, thereby reshaping immunosuppressive TME for cancer treatment, has great potential as an immunogene therapy in clinical applications.
Keywords: CKb11; Immune checkpoint PD-1/PD-L1; Immunogene therapy; Nanomedicine; Ovarian cancer.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Non-viral vector mediated CKb11 with folic acid modification regulates macrophage polarization and DC maturation to elicit immune response against cancer.Bioact Mater. 2021 Apr 6;6(11):3678-3691. doi: 10.1016/j.bioactmat.2021.03.031. eCollection 2021 Nov. Bioact Mater. 2021. PMID: 33898872 Free PMC article.
-
Functionalized biomimetic nanoparticles combining programmed death-1/programmed death-ligand 1 blockade with photothermal ablation for enhanced colorectal cancer immunotherapy.Acta Biomater. 2023 Feb;157:451-466. doi: 10.1016/j.actbio.2022.11.043. Epub 2022 Nov 25. Acta Biomater. 2023. PMID: 36442821
-
Acidosis-mediated increase in IFN-γ-induced PD-L1 expression on cancer cells as an immune escape mechanism in solid tumors.Mol Cancer. 2023 Dec 15;22(1):207. doi: 10.1186/s12943-023-01900-0. Mol Cancer. 2023. PMID: 38102680 Free PMC article.
-
Augmenting Anticancer Immunity Through Combined Targeting of Angiogenic and PD-1/PD-L1 Pathways: Challenges and Opportunities.Front Immunol. 2020 Nov 5;11:598877. doi: 10.3389/fimmu.2020.598877. eCollection 2020. Front Immunol. 2020. PMID: 33250900 Free PMC article. Review.
-
Recent advances in tumor microenvironment-targeted nanomedicine delivery approaches to overcome limitations of immune checkpoint blockade-based immunotherapy.J Control Release. 2021 Apr 10;332:109-126. doi: 10.1016/j.jconrel.2021.02.002. Epub 2021 Feb 8. J Control Release. 2021. PMID: 33571549 Review.
Cited by
-
NIR-triggered programmable nanomotor with H2S and NO generation for cascading oncotherapy by three-pronged reinforcing ICD.Mater Today Bio. 2025 Feb 3;31:101540. doi: 10.1016/j.mtbio.2025.101540. eCollection 2025 Apr. Mater Today Bio. 2025. PMID: 39995577 Free PMC article.
-
Nanotechnology for boosting ovarian cancer immunotherapy.J Ovarian Res. 2024 Oct 14;17(1):202. doi: 10.1186/s13048-024-01507-z. J Ovarian Res. 2024. PMID: 39402681 Free PMC article. Review.
-
Ultrasound-responsive nanocarriers with siRNA and Fe3O4 regulate macrophage polarization and phagocytosis for augmented non-small cell lung cancer immunotherapy.J Nanobiotechnology. 2024 Oct 7;22(1):605. doi: 10.1186/s12951-024-02883-w. J Nanobiotechnology. 2024. PMID: 39375761 Free PMC article.
References
-
- Lheureux S., Braunstein M., Oza A.M. Epithelial ovarian cancer: evolution of management in the era of precision medicine. CA A Cancer J. Clin. 2019;69(4):280–304. - PubMed
-
- Kuroki L., Guntupalli S.R. Treatment of epithelial ovarian cancer. Br. Med. J. 2020;371:m3773. - PubMed
-
- Armstrong D.K., Alvarez R.D., Backes F.J., Bakkum-Gamez J.N., Barroilhet L., Behbakht K., Berchuck A., Chen L.M., Chitiyo V.C., Cristea M., DeRosa M., Eisenhauer E.L., Gershenson D.M., Gray H.J., Grisham R., Hakam A., Jain A., Karam A., Konecny G.E., Leath C.A., III, Leiserowitz G., Liu J., Martin L., Matei D., McHale M., McLean K., Miller D.S., Percac-Lima S., Remmenga S.W., Schorge J., Stewart D., Thaker P.H., Vargas R., Hendrickson A.W., Werner T.L., Zsiros E., Dwyer M.A., Hang L. NCCN guidelines(R) insights: ovarian cancer, version 3.2022. J. Natl. Compr. Cancer Netw. : J. Natl. Compr. Cancer Netw. 2022;20(9):972–980. - PubMed
-
- Gardner G.J., Chi D.S. Recurrent ovarian cancer - sculpting a promising future with surgery. N. Engl. J. Med. 2021;385(23):2187–2188. - PubMed
-
- Schoutrop E., Moyano-Galceran L., Lheureux S., Mattsson J., Lehti K., Dahlstrand H., Magalhaes I. Molecular, cellular and systemic aspects of epithelial ovarian cancer and its tumor microenvironment. Semin. Cancer Biol. 2022;86(Pt 3):207–223. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
