

Patient-Reported and Clinical Outcomes of Surgically Treated Patients With Symptomatic Spinal Metastases: Results From Epidemiology, Process, and Outcomes of Spine Oncology (EPOSO), a Prospective, Multi-Institutional and International Study
- PMID: 38832791
- PMCID: PMC11449425
- DOI: 10.1227/neu.0000000000002989
Patient-Reported and Clinical Outcomes of Surgically Treated Patients With Symptomatic Spinal Metastases: Results From Epidemiology, Process, and Outcomes of Spine Oncology (EPOSO), a Prospective, Multi-Institutional and International Study
Abstract
Background and objectives: The palliative impact of spine surgery for metastatic disease is evolving with improvements in surgical technique and multidisciplinary cancer care. The goal of this study was to prospectively evaluate long-term clinical outcomes including health-related quality-of-life (HRQOL) measures, using spine cancer-specific patient-reported-outcome (PRO) measures, in patients with symptomatic spinal metastases who underwent surgical management.
Methods: The Epidemiology, Process, and Outcomes of Spine Oncology (EPOSO, ClinicalTrials.gov identifier: NCT01825161) trial is a prospective-observational cohort study that included 10 specialist centers in North America and Europe. Patients aged 18 to 75 years who underwent surgery for spinal metastases were included. Prospective assessments included both spine tumor-specific and generic PRO tools which were collected for a minimum of 2 years post-treatment or until death.
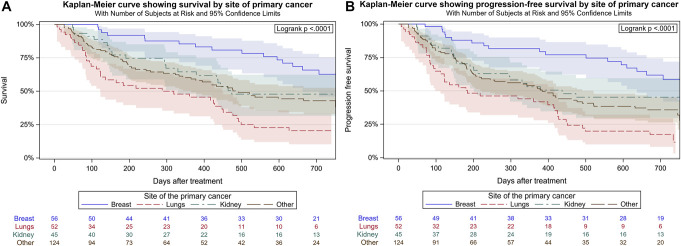
Results: Two hundred and eighty patients (51.8% female, mean age 57.9 years) were included. At presentation, the mean Charlson Comorbidity Index was 6.0, 35.7% had neurological deficits as defined by the American Spinal Cord Injury Association scores, 47.2% had high-grade epidural spinal cord compression (2-3), and 89.6% had impending or frank instability as measured by a Spinal Instability Neoplastic Score of ≥7. The most common primary tumor sites were breast (20.2%), lung (18.8%), kidney (16.2%), and prostate (6.5%). The median overall survival postsurgery was 501 days, and the 2-year progression-free-survival rate was 38.4%. Compared with baseline, significant and durable improvements in HRQOL were observed at the 6-week, 12-week, 26-week, 1-year, and 2-year follow-up assessments from a battery of PRO questionnaires including the spine cancer-specific, validated, Spine Oncology Study Group Outcomes Questionnaire v2.0, the Short Form 36 version 2, EuroQol-5 Dimension (3L), and pain numerical rating scale score.
Conclusion: Multi-institutional, prospective-outcomes data confirm that surgical decompression and/or stabilization provides meaningful and durable improvements in multiple HRQOL domains, including spine-specific outcomes based on the Spine Oncology Study Group Outcomes Questionnaire v2.0, for patients with metastatic spine disease.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Congress of Neurological Surgeons.
Figures


References
-
- Cobb CA, 3rd, Leavens ME, Eckles N. Indications for nonoperative treatment of spinal cord compression due to breast cancer. J Neurosurg. 1977;47(5):653-658. - PubMed
-
- Wong DA, Fornasier VL, MacNab I. Spinal metastases: the obvious, the occult, and the impostors. Spine (Phila Pa 1976). 1990;15(1):1-4. - PubMed
-
- Klimo P, Jr., Schmidt MH. Surgical management of spinal metastases. Oncologist. 2004;9(2):188-196. - PubMed
-
- North RB, LaRocca VR, Schwartz J, et al. Surgical management of spinal metastases: analysis of prognostic factors during a 10-year experience. J Neurosurg Spine. 2005;2(5):564-573. - PubMed
-
- Sinson GP, Zager EL. Metastases and spinal cord compression. N Engl J Med. 1992;327(27):1953-1955; author reply 1954-1955. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
