

Radiation-Induced DNA Damage in Uveal Melanoma Is Influenced by Dose Delivery and Chromosome 3 Status
- PMID: 38833258
- PMCID: PMC11156202
- DOI: 10.1167/iovs.65.6.7
Radiation-Induced DNA Damage in Uveal Melanoma Is Influenced by Dose Delivery and Chromosome 3 Status
Abstract
Purpose: The purpose of this study was to analyze the extent of DNA breaks in primary uveal melanoma (UM) with regard to radiotherapy dose delivery (single-dose versus fractionated) and monosomy 3 status.
Methods: A total of 54 patients with UM were included. Stereotactic radiotherapy (SRT) was performed in 23 patients, with 8 undergoing single-dose SRT (sdSRT) treatment and 15 receiving fractionated SRT (fSRT). DNA breaks in the enucleated or endoresected tumors were visualized by a TUNEL assay and quantified by measuring the TUNEL-positive area. Protein expression was analyzed by immunohistochemistry. Co-detection of chromosome 3 with proteins was performed by immuno-fluorescent in situ hybridization.
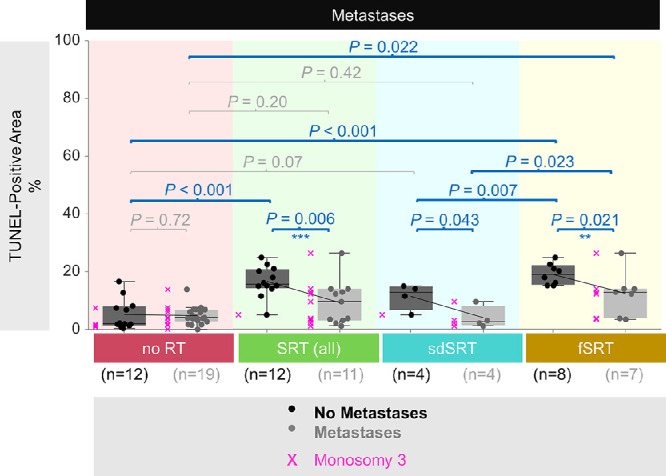
Results: The amount of DNA breaks in the total irradiated group was increased by 2.7-fold (P < 0.001) compared to non-irradiated tissue. Tumors treated with fSRT were affected more severely, showing 2.1-fold more DNA damage (P = 0.007) compared to the cases after single (high) dose irradiation (sdSRT). Monosomy 3 tumors showed less DNA breaks compared to disomy 3 samples (P = 0.004). The presence of metastases after radiotherapy correlated with monosomy 3 and less DNA breaks compared to patients with non-metastatic cancer in the combined group with fSRT and sdSRT (P < 0.05).
Conclusions: Fractionated irradiation led to more DNA damage than single-dose treatment in primary UM. As tumors with monosomy 3 showed less DNA breaks than those with disomy 3, this may indicate that they are less radiosensitive, which may influence the efficacy of irradiation.
Conflict of interest statement
Disclosure:
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
