

Predicting cardiovascular disease risk using photoplethysmography and deep learning
- PMID: 38833495
- PMCID: PMC11149850
- DOI: 10.1371/journal.pgph.0003204
Predicting cardiovascular disease risk using photoplethysmography and deep learning
Abstract
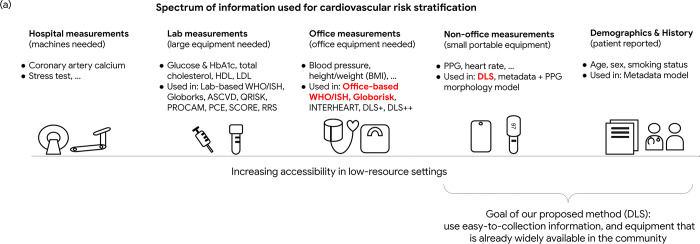
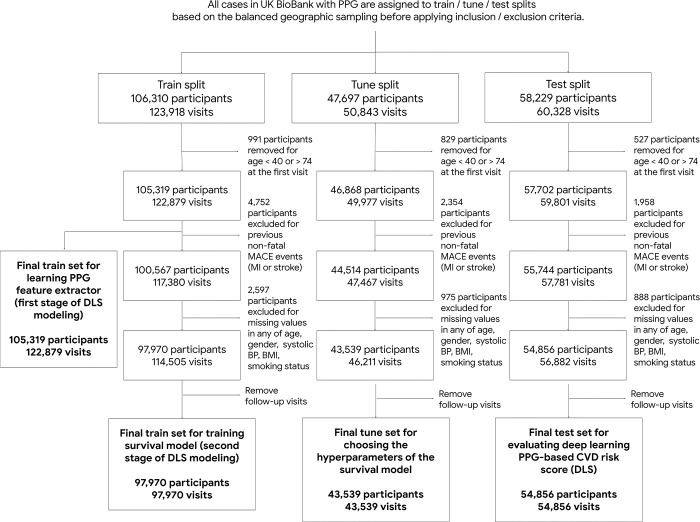
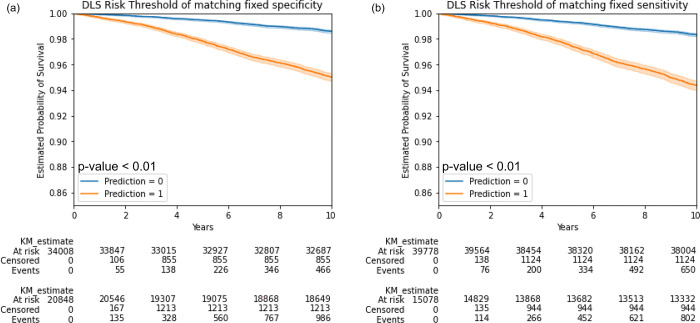
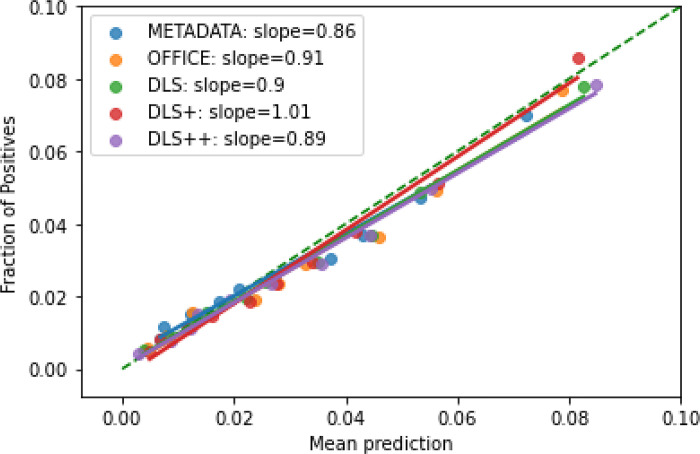
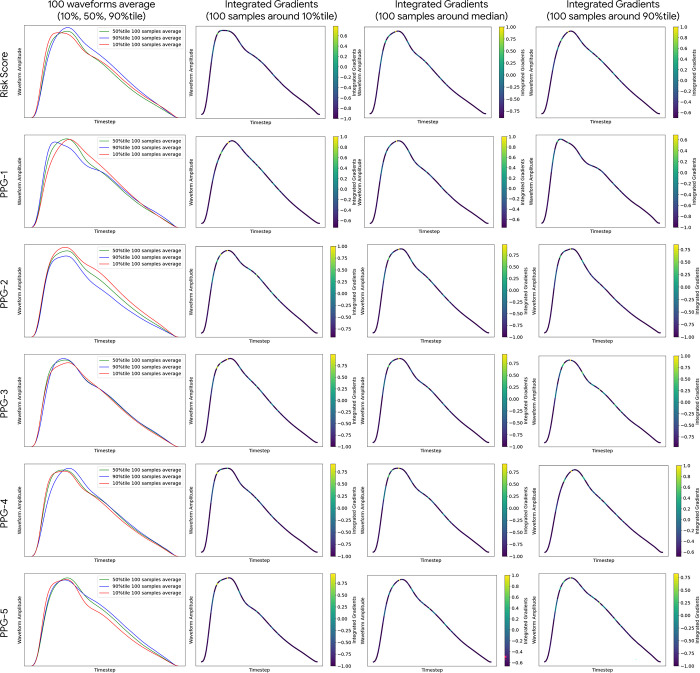
Cardiovascular diseases (CVDs) are responsible for a large proportion of premature deaths in low- and middle-income countries. Early CVD detection and intervention is critical in these populations, yet many existing CVD risk scores require a physical examination or lab measurements, which can be challenging in such health systems due to limited accessibility. We investigated the potential to use photoplethysmography (PPG), a sensing technology available on most smartphones that can potentially enable large-scale screening at low cost, for CVD risk prediction. We developed a deep learning PPG-based CVD risk score (DLS) to predict the probability of having major adverse cardiovascular events (MACE: non-fatal myocardial infarction, stroke, and cardiovascular death) within ten years, given only age, sex, smoking status and PPG as predictors. We compare the DLS with the office-based refit-WHO score, which adopts the shared predictors from WHO and Globorisk scores (age, sex, smoking status, height, weight and systolic blood pressure) but refitted on the UK Biobank (UKB) cohort. All models were trained on a development dataset (141,509 participants) and evaluated on a geographically separate test (54,856 participants) dataset, both from UKB. DLS's C-statistic (71.1%, 95% CI 69.9-72.4) is non-inferior to office-based refit-WHO score (70.9%, 95% CI 69.7-72.2; non-inferiority margin of 2.5%, p<0.01) in the test dataset. The calibration of the DLS is satisfactory, with a 1.8% mean absolute calibration error. Adding DLS features to the office-based score increases the C-statistic by 1.0% (95% CI 0.6-1.4). DLS predicts ten-year MACE risk comparable with the office-based refit-WHO score. Interpretability analyses suggest that the DLS-extracted features are related to PPG waveform morphology and are independent of heart rate. Our study provides a proof-of-concept and suggests the potential of a PPG-based approach strategies for community-based primary prevention in resource-limited regions.
Copyright: © 2024 Weng et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
Author WHW, SB, MD, CC, SK, YL, and DA are employed at Google LLC and hold shares in Alphabet, and are co-inventors on patents (in various stages) for CVD risk prediction using deep learning and PPG, but declare no non-financial competing interests. LH, BB, CYM, YM, GSC, SS, SP are employed at Google LLC and hold shares in Alphabet but declare no non-financial competing interests. SK serves as an Associate Editor for this journal but had no role to play in the editorial process and decisions for this manuscript. GD declares no financial or non-financial competing interests.
Figures
Similar articles
-
Laboratory-based and office-based Globorisk scores to predict 10-year risk of cardiovascular diseases among Iranians: results from the Fasa PERSIAN cohort.BMC Med Res Methodol. 2022 Nov 26;22(1):305. doi: 10.1186/s12874-022-01791-7. BMC Med Res Methodol. 2022. PMID: 36435774 Free PMC article.
-
Development and Validation of a Protein-Based Risk Score for Cardiovascular Outcomes Among Patients With Stable Coronary Heart Disease.JAMA. 2016 Jun 21;315(23):2532-41. doi: 10.1001/jama.2016.5951. JAMA. 2016. PMID: 27327800
-
Performance of the SCORE and Globorisk cardiovascular risk prediction models: a prospective cohort study in Dutch general practice.Br J Gen Pract. 2022 Dec 21;73(726):e24-e33. doi: 10.3399/BJGP.2021.0726. Print 2023 Jan. Br J Gen Pract. 2022. PMID: 36443066 Free PMC article.
-
Derivation, internal validation, and recalibration of a cardiovascular risk score for Latin America and the Caribbean (Globorisk-LAC): A pooled analysis of cohort studies.Lancet Reg Health Am. 2022 May;9:None. doi: 10.1016/j.lana.2022.100258. Lancet Reg Health Am. 2022. PMID: 35711683 Free PMC article.
-
Blood pressure estimation and classification using a reference signal-less photoplethysmography signal: a deep learning framework.Phys Eng Sci Med. 2023 Dec;46(4):1589-1605. doi: 10.1007/s13246-023-01322-8. Epub 2023 Sep 25. Phys Eng Sci Med. 2023. PMID: 37747644
Cited by
-
Deep learning approaches for assessing pediatric sleep apnea severity through SpO2 signals.Sci Rep. 2024 Oct 1;14(1):22696. doi: 10.1038/s41598-024-67729-9. Sci Rep. 2024. PMID: 39353980 Free PMC article.
-
Predicting cardiovascular risk with hybrid ensemble learning and explainable AI.Sci Rep. 2025 May 23;15(1):17927. doi: 10.1038/s41598-025-01650-7. Sci Rep. 2025. PMID: 40410273 Free PMC article.
References
-
- Cardiovascular diseases (CVDs). [cited 17 Oct 2022]. Available: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases...
-
- Ueda P, Woodward M, Lu Y, Hajifathalian K, Al-Wotayan R, Aguilar-Salinas CA, et al.. Laboratory-based and office-based risk scores and charts to predict 10-year risk of cardiovascular disease in 182 countries: a pooled analysis of prospective cohorts and health surveys. Lancet Diabetes Endocrinol. 2017;5: 196–213. doi: 10.1016/S2213-8587(17)30015-3 - DOI - PMC - PubMed
-
- Lloyd-Jones DM, Huffman MD, Karmali KN, Sanghavi DM, Wright JS, Pelser C, et al.. Estimating Longitudinal Risks and Benefits From Cardiovascular Preventive Therapies Among Medicare Patients: The Million Hearts Longitudinal ASCVD Risk Assessment Tool: A Special Report From the American Heart Association and American College of Cardiology. Circulation. 2017;135: e793–e813. doi: 10.1161/CIR.0000000000000467 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous