

Prevalence and Impact of Bypassing or Overriding Phase 2 Trials in Neurologic Drug Development
- PMID: 38833654
- PMCID: PMC11226307
- DOI: 10.1212/WNL.0000000000209533
Prevalence and Impact of Bypassing or Overriding Phase 2 Trials in Neurologic Drug Development
Abstract
Background and objectives: Pivotal trials for neurologic drugs in clinical development are often initiated without a phase 2 trial ("bypass") or despite a negative phase 2 efficacy result ("override"). Such practices may degrade the risk/benefit ratio of phase 3 trials. The aim of this study is to estimate the proportion of phase 3 trials for 10 neurologic diseases started without a positive phase 2 trial, to identify factors associated with this practice, and to investigate any association with unfavorable phase 3 trial outcomes.
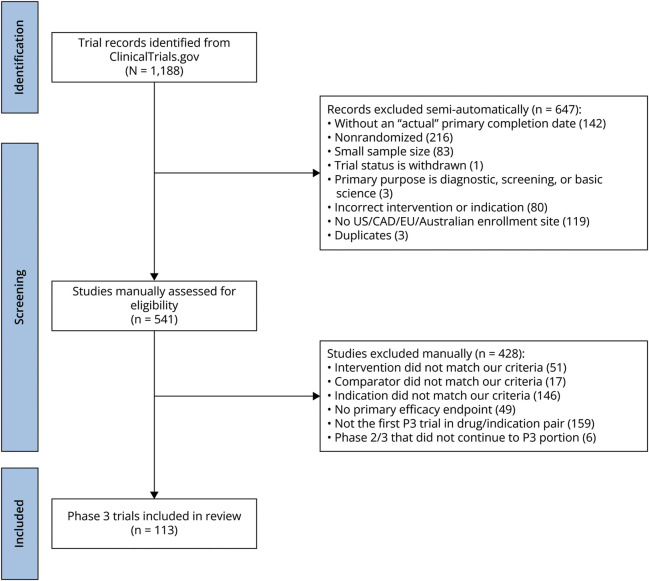
Methods: We searched ClinicalTrials.gov for phase 3 trials completed during 2011-2021, with at least 1 research site in the United States, Canada, the European Union, the United Kingdom, or Australia, and investigating drugs or biologics for treatment of 10 neurologic conditions. Our primary objective was to assess the prevalence of phase 2 bypass/override by searching for preceding phase 2 trials. We used Fisher exact tests to determine whether phase 3 trial characteristics and trial results were associated with phase 2 bypass/override.
Results: Of the 1,188 phase 3 trials captured in our search, 113 met eligibility for inclusion. Of these, 46% were not preceded by a phase 2 trial that was positive on an efficacy endpoint (31% bypassed and 15% overrode phase 2 trial). Phase 2 bypass/override was not associated with industry funding (77% vs 89%, 95% CI 0.75-7.55, p = 0.13) or testing already approved interventions (23% vs 15%, 95% CI 0.60-5.14, p = 0.33). Overall, phase 3 trials based on phase 2 bypassed/override were statistically significantly less likely to be positive on their primary outcome (31% vs 57%, respectively, 95% CI 1.21-6.92, p = 0.01). This effect disappeared when indications characterized by nearly universal positive or negative results were excluded. Trials that bypassed/overrode phase 2 trials were not statistically significantly more likely to be terminated early because of safety or futility (29% vs 15%, respectively, 95% CI 0.15-1.18, p = 0.11) and did not show increased risk of adverse events in experimental arms (RR = 1.46, 95% CI 1.19-1.79, vs RR = 1.36, 95% CI 1.10-1.69, respectively, p = 0.65).
Discussion: Almost half of the neurologic disease phase 3 trials were initiated without the support of a positive phase 2 trial. Although our analysis does not establish harm with bypass/override, its prevalence and the scientific rationale for phase 2 trial testing favor development of criteria defining when phase 2 bypass/override is justified.
Conflict of interest statement
J. Kimmelman received consulting fees from Amylyx Inc. The other authors declare no other relevant disclosures. Go to
Figures
Similar articles
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
References
-
- O'Neill GN. Unique challenges in the development of therapies for neurological disorders. In: Ravina B, Cummings J, McDermott M, Poole RM, eds. Clinical Trials in Neurology: Design, Conduct, Analysis. Cambridge University Press; 2012:19-27. doi: 10.1017/CBO9781139032445.004 - DOI
-
- Feltner DE, Evans KR. Phase II development and the path to personalized medicine in CNS disease. In: Kalali A, Preskorn S, Kwentus J, et al., Essential CNS Drug Development. 2012:70-91. doi: 10.1017/CBO9780511977640.006 - DOI
-
- Kimmelman J. Ethics in clinical trials involving the central nervous system: risk, benefit, justice, and integrity. In: Ravina B, Cummings J, McDermott M, Poole RM, eds. Clinical Trials in Neurology: Design, Conduct, Analysis. Cambridge University Press; 2012:173-186. doi: 10.1017/CBO9781139032445.017 - DOI
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous