

Personalized bacteriophage therapy outcomes for 100 consecutive cases: a multicentre, multinational, retrospective observational study
- PMID: 38834776
- PMCID: PMC11153159
- DOI: 10.1038/s41564-024-01705-x
Personalized bacteriophage therapy outcomes for 100 consecutive cases: a multicentre, multinational, retrospective observational study
Abstract
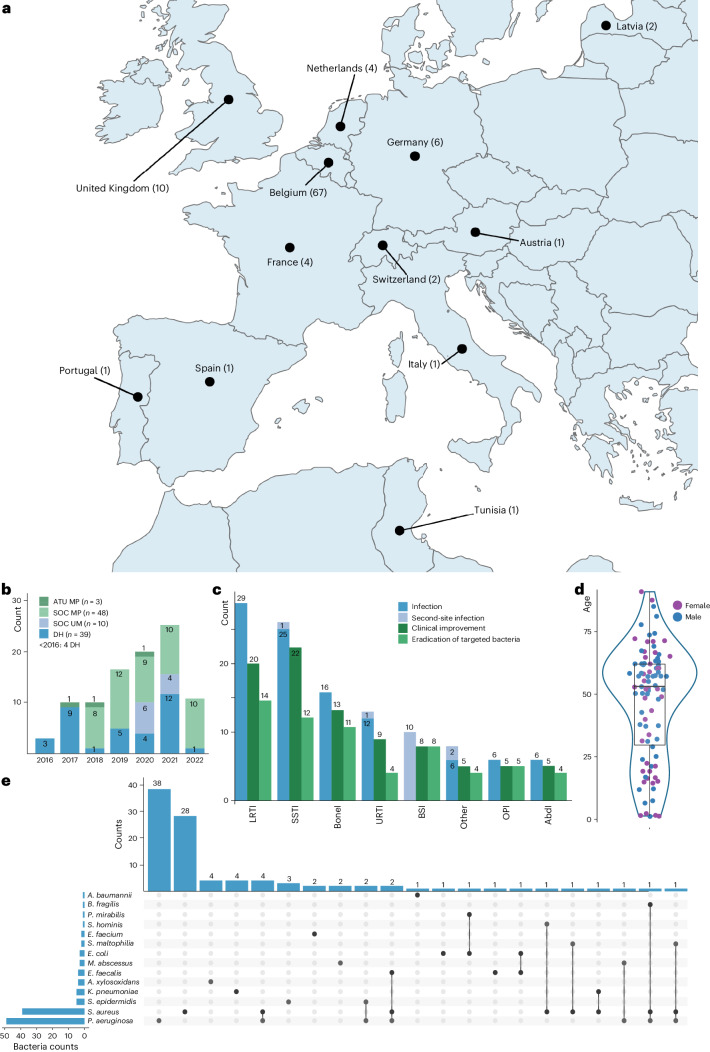
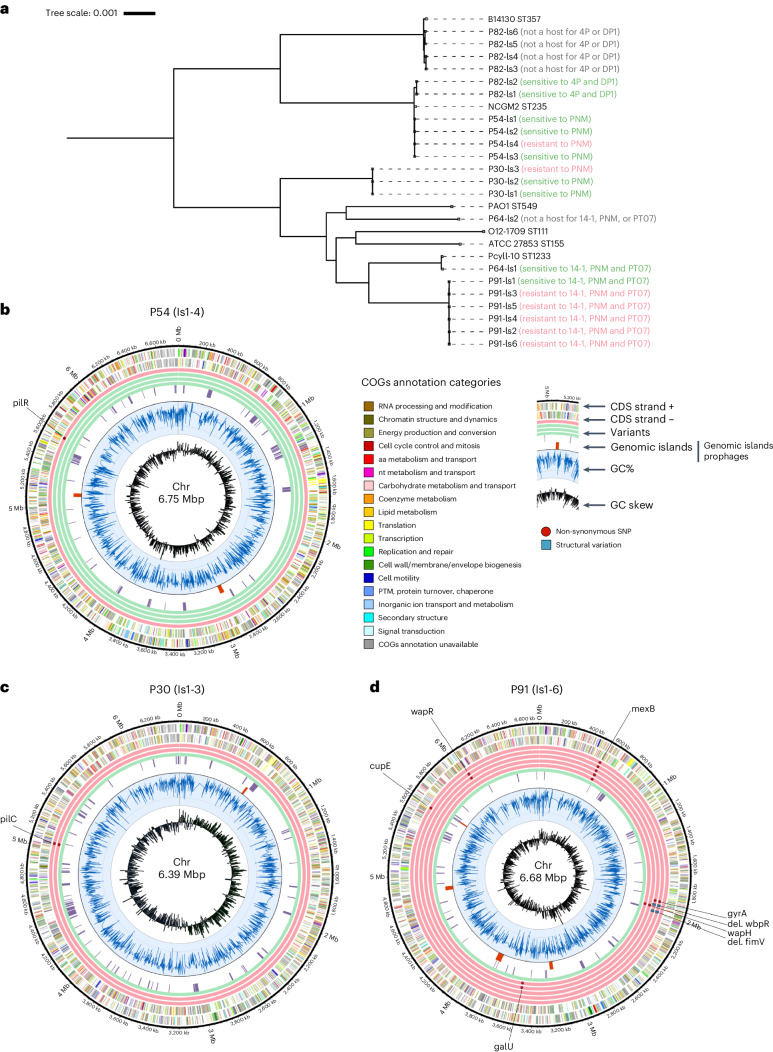
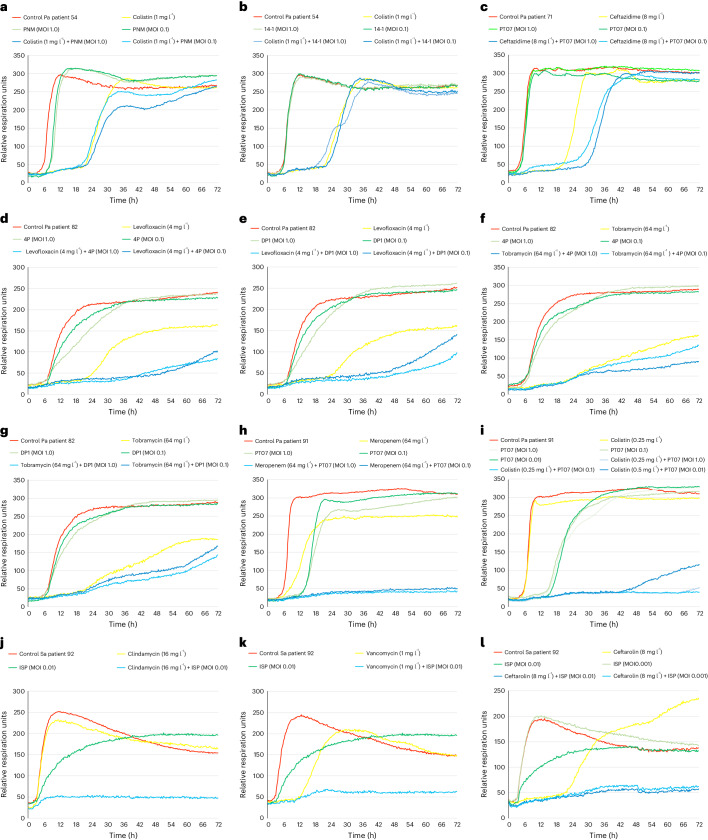
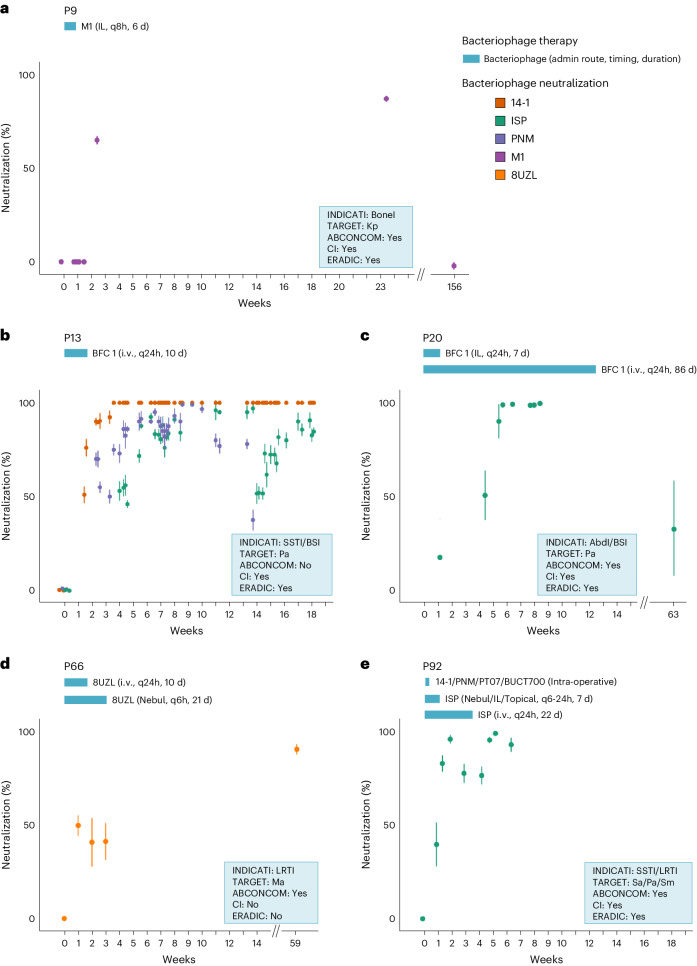
In contrast to the many reports of successful real-world cases of personalized bacteriophage therapy (BT), randomized controlled trials of non-personalized bacteriophage products have not produced the expected results. Here we present the outcomes of a retrospective observational analysis of the first 100 consecutive cases of personalized BT of difficult-to-treat infections facilitated by a Belgian consortium in 35 hospitals, 29 cities and 12 countries during the period from 1 January 2008 to 30 April 2022. We assessed how often personalized BT produced a positive clinical outcome (general efficacy) and performed a regression analysis to identify functional relationships. The most common indications were lower respiratory tract, skin and soft tissue, and bone infections, and involved combinations of 26 bacteriophages and 6 defined bacteriophage cocktails, individually selected and sometimes pre-adapted to target the causative bacterial pathogens. Clinical improvement and eradication of the targeted bacteria were reported for 77.2% and 61.3% of infections, respectively. In our dataset of 100 cases, eradication was 70% less probable when no concomitant antibiotics were used (odds ratio = 0.3; 95% confidence interval = 0.127-0.749). In vivo selection of bacteriophage resistance and in vitro bacteriophage-antibiotic synergy were documented in 43.8% (7/16 patients) and 90% (9/10) of evaluated patients, respectively. We observed a combination of antibiotic re-sensitization and reduced virulence in bacteriophage-resistant bacterial isolates that emerged during BT. Bacteriophage immune neutralization was observed in 38.5% (5/13) of screened patients. Fifteen adverse events were reported, including seven non-serious adverse drug reactions suspected to be linked to BT. While our analysis is limited by the uncontrolled nature of these data, it indicates that BT can be effective in combination with antibiotics and can inform the design of future controlled clinical trials. BT100 study, ClinicalTrials.gov registration: NCT05498363 .
© 2024. The Author(s).
Conflict of interest statement
R.N.-P. has been a scientific consultant for BiomX Inc., and has participated and served as a principal investigator and member of Data Safety Monitoring Boards for a clinical trial by Technophage S. A. M.D.L. and N.C. are co-founders of the startup Fagoterapia Lab s.r.l. T.F. is the principal investigator of the PhagoDAIR I study and is consultant for PHAXIAM to conceive clinical trials (no direct funding, contract signed with hospices Civils de Lyon). R.N.-.P, S.M., T.F. and J.-P.P., respectively, serve as Chair, Secretary, Education Officer/Clinical Officer and Science Officer of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Study Group for Non-Traditional Antibacterial Therapy (ESGNTA), Basel, Switzerland.
Figures




References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
