

An in-depth analysis of young adults with osteonecrosis secondary to developmental dysplasia of the hip who underwent total hip arthroplasty
- PMID: 38835008
- PMCID: PMC11149231
- DOI: 10.1186/s12891-024-07517-8
An in-depth analysis of young adults with osteonecrosis secondary to developmental dysplasia of the hip who underwent total hip arthroplasty
Abstract
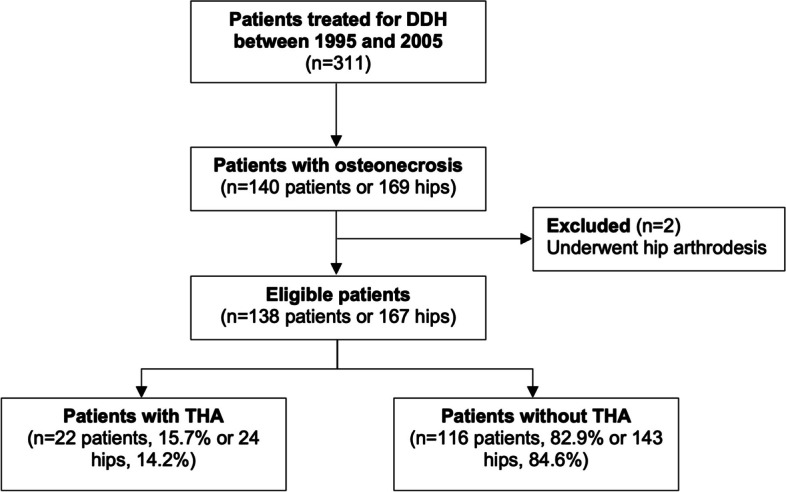
Background: Patients with osteonecrosis of the femoral head secondary to DDH frequently require total hip arthroplasty (THA), but it is not well understood which factors necessitate this requirement. We determined the incidence of THA in patients who have osteonecrosis secondary to DDH and factors associated with need for THA.
Methods: We included patients who received closed or open reductions between 1995 and 2005 with subsequent development of osteonecrosis. We determined osteonecrosis according to Bucholz and Ogden; osteoarthritis severity (Kellgren-Lawrence), subluxation (Shenton's line); neck-shaft angle; and acetabular dysplasia (centre-edge and Sharp angles). We also recorded the number of operations of the hip in childhood and reviewed case notes of patients who received THA to describe clinical findings prior to THA. We assessed the association between radiographic variables and the need for THA using univariate logistic regression.
Results: Of 140 patients (169 hips), 22 patients received 24 THA (14%) at a mean age of 21.3 ± 3.7 years. Associated with the need for THA were grade III osteonecrosis (OR 4.25; 95% CI 1.70-10.77; p = 0.0019), grade IV osteoarthritis (21.8; 7.55-68.11; p < 0.0001) and subluxation (8.22; 2.91-29.53; p = 0.0003). All patients who required THA reported at least 2 of: severe pain including at night, stiffness, and reduced mobility. Acetabular dysplasia and number of previous operations were not associated with the need for THA.
Conclusions: We identified a 14% incidence of THA by age 34 years in patients with osteonecrosis secondary to DDH. Grade III osteonecrosis (global involvement femoral head and neck) was strongly associated with THA, emphasising the importance to avoid osteonecrosis when treating DDH.
Keywords: DDH; Osteonecrosis; Total hip arthroplasty.
© 2024. Crown.
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
The John Charnley Award: Redefining the Natural History of Osteoarthritis in Patients With Hip Dysplasia and Impingement.Clin Orthop Relat Res. 2017 Feb;475(2):336-350. doi: 10.1007/s11999-016-4815-2. Clin Orthop Relat Res. 2017. PMID: 27071391 Free PMC article.
-
Patient-reported outcomes in young adults with osteonecrosis secondary to developmental dysplasia of the hip - a longitudinal and cross-sectional evaluation.BMC Musculoskelet Disord. 2021 Jan 7;22(1):42. doi: 10.1186/s12891-020-03865-3. BMC Musculoskelet Disord. 2021. PMID: 33413228 Free PMC article.
-
One-third of Hips After Periacetabular Osteotomy Survive 30 Years With Good Clinical Results, No Progression of Arthritis, or Conversion to THA.Clin Orthop Relat Res. 2017 Apr;475(4):1154-1168. doi: 10.1007/s11999-016-5169-5. Clin Orthop Relat Res. 2017. PMID: 27905061 Free PMC article.
-
Does Cup Position at the High Hip Center or Anatomic Hip Center in THA for Developmental Dysplasia of the Hip Result in Better Harris Hip Scores and Revision Incidence? A Systematic Review.Clin Orthop Relat Res. 2021 May 1;479(5):1119-1130. doi: 10.1097/CORR.0000000000001618. Clin Orthop Relat Res. 2021. PMID: 33539054 Free PMC article.
-
Challenges in Total Hip Arthroplasty in the Setting of Developmental Dysplasia of the Hip.J Arthroplasty. 2017 Sep;32(9S):S38-S44. doi: 10.1016/j.arth.2017.02.024. Epub 2017 Feb 22. J Arthroplasty. 2017. PMID: 28291651 Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
