

In-situ Audiometry Compared to Conventional Audiometry for Hearing Aid Fitting
- PMID: 38835268
- PMCID: PMC11155351
- DOI: 10.1177/23312165241259704
In-situ Audiometry Compared to Conventional Audiometry for Hearing Aid Fitting
Abstract
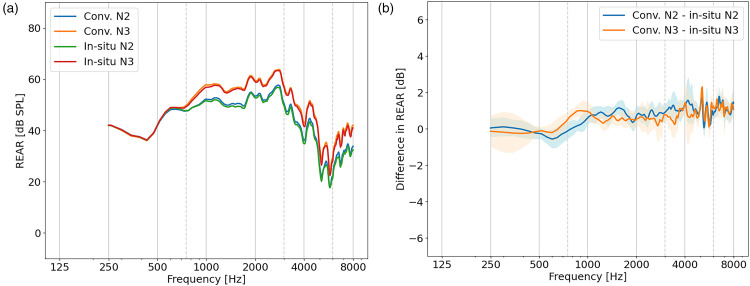
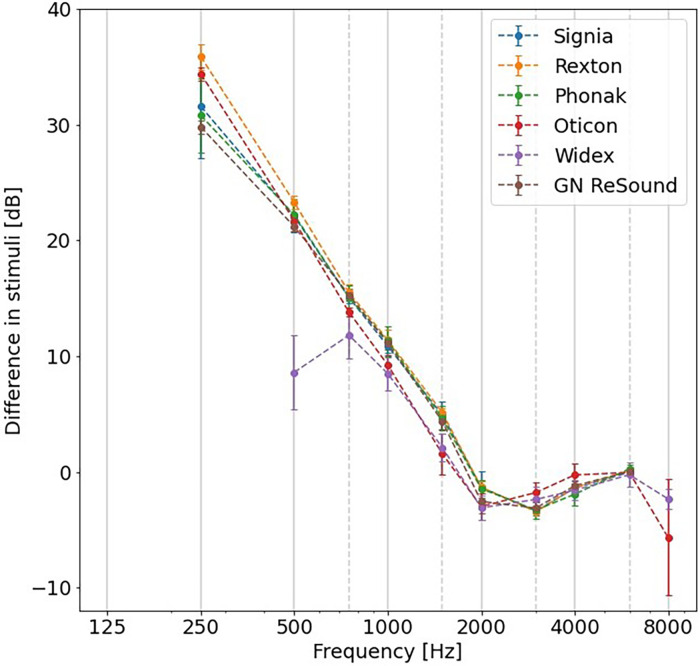
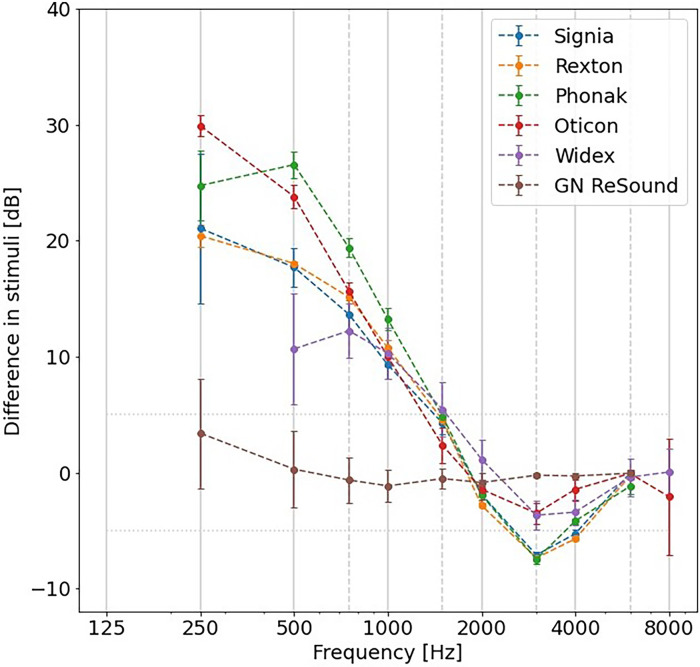
The use of in-situ audiometry for hearing aid fitting is appealing due to its reduced resource and equipment requirements compared to standard approaches employing conventional audiometry alongside real-ear measures. However, its validity has been a subject of debate, as previous studies noted differences between hearing thresholds measured using conventional and in-situ audiometry. The differences were particularly notable for open-fit hearing aids, attributed to low-frequency leakage caused by the vent. Here, in-situ audiometry was investigated for six receiver-in-canal hearing aids from different manufacturers through three experiments. In Experiment I, the hearing aid gain was measured to investigate whether corrections were implemented to the prescribed target gain. In Experiment II, the in-situ stimuli were recorded to investigate if corrections were directly incorporated to the delivered in-situ stimulus. Finally, in Experiment III, hearing thresholds using in-situ and conventional audiometry were measured with real patients wearing open-fit hearing aids. Results indicated that (1) the hearing aid gain remained unaffected when measured with in-situ or conventional audiometry for all open-fit measurements, (2) the in-situ stimuli were adjusted for up to 30 dB at frequencies below 1000 Hz for all open-fit hearing aids except one, which also recommends the use of closed domes for all in-situ measurements, and (3) the mean interparticipant threshold difference fell within 5 dB for frequencies between 250 and 6000 Hz. The results clearly indicated that modern measured in-situ thresholds align (within 5 dB) with conventional thresholds measured, indicating the potential of in-situ audiometry for remote hearing care.
Keywords: auditory rehabilitation; connected hearing care; in-situ audiometry; remote hearing aid fitting; tele audiology.
Conflict of interest statement
Declaration of Conflicting InterestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

Similar articles
-
Comparing Self-Fitting Strategies for Over-the-Counter Hearing Aids: A Crossover Clinical Trial.JAMA Otolaryngol Head Neck Surg. 2024 Sep 1;150(9):784-791. doi: 10.1001/jamaoto.2024.2007. JAMA Otolaryngol Head Neck Surg. 2024. PMID: 39052241 Free PMC article. Clinical Trial.
-
Validation of an In Situ Self-Administered Hearing Test with a Self-Fitting Device for Mild to Moderately Severe Hearing Loss in Various Acoustic Environments.Ann Otol Rhinol Laryngol. 2025 Jul;134(7):502-510. doi: 10.1177/00034894251325617. Epub 2025 Mar 12. Ann Otol Rhinol Laryngol. 2025. PMID: 40071674
-
Mobile audiometry for hearing threshold assessment: A systematic review and meta-analysis.Clin Otolaryngol. 2024 Jan;49(1):74-86. doi: 10.1111/coa.14107. Epub 2023 Oct 12. Clin Otolaryngol. 2024. PMID: 37828806
-
Interventions to improve hearing aid use in adult auditory rehabilitation.Cochrane Database Syst Rev. 2016 Aug 18;2016(8):CD010342. doi: 10.1002/14651858.CD010342.pub3. Cochrane Database Syst Rev. 2016. PMID: 27537242 Free PMC article.
-
Bone-anchored hearing aids (BAHAs) for people who are bilaterally deaf: a systematic review and economic evaluation.Health Technol Assess. 2011 Jul;15(26):1-200, iii-iv. doi: 10.3310/hta15260. Health Technol Assess. 2011. PMID: 21729632 Free PMC article.
Cited by
-
Development and Validation of a Self-Administered Online Hearing Test.Trends Hear. 2025 Jan-Dec;29:23312165251317923. doi: 10.1177/23312165251317923. Epub 2025 Mar 18. Trends Hear. 2025. PMID: 40101250 Free PMC article.
References
-
- American Speech and Hearing Association (2023). Hearing Aids For Adults. Https://Www.Asha.Org/Practice-Portal/Professional-Issues/Hearing-Aids-fo....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
