

Our 7-year experience supporting the Ross autograft with the novel technique of Personalized External Aortic Root Support
- PMID: 38835595
- PMCID: PMC11145418
- DOI: 10.1016/j.xjtc.2024.02.004
Our 7-year experience supporting the Ross autograft with the novel technique of Personalized External Aortic Root Support
Abstract
Objective: The Ross operation is a widely accepted option for aortic valve replacement in children, and evidence shows its excellent results in terms of hemodynamics and durability. However, indications are still limited due to the fact that it is a technically demanding procedure, only performed by specialized surgeons. On top of that, and despite numerous techniques being applied, autograft dilatation remains a key disadvantage, which can lead to graft failure. In recent years, the ExoVasc Personalized External Aortic Root Support (PEARS) has proven to be a safe and effective option to prevent aortic root dilatation in various aortopathies and is a technique that lends itself to support the pulmonary autograft in the Ross operation.
Methods: During the past 7 years, we have used the ExoVasc PEARS graft, manufactured from the patients' pulmonary artery measurements from computed tomography scan data, to support the pulmonary autograft in the Ross operation. This graft (manufactured by Exstent Ltd, UK) is implanted at the same time as the autograft. We have reviewed all the patients who underwent this surgery, including demographic data, aorta measurements, operative data, and follow-up assessment consisting of periodic echocardiograms and magnetic resonance imaging scans.
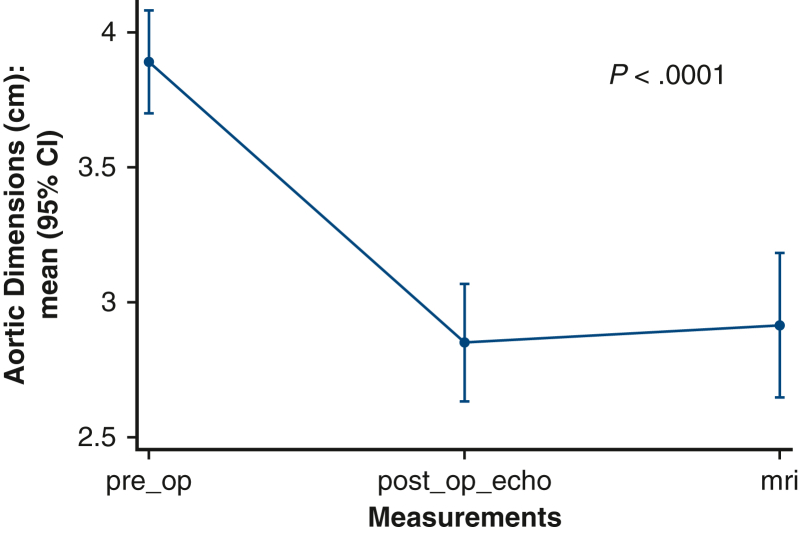
Results: Fifty patients were included in the study. Mean age at the time of the operation was 29.84 years, the youngest patient was 9 years-old. Nineteen patients (38%) had previous sternotomies; 11 of them having had a previous aortic valve replacement. Seventy-two percent of patients had initially a bicuspid aortic valve. Mean diameter of the ascending aorta was 3.83 cm. Forty-four percent of patients required a concomitant reduction aortoplasty due to mismatch sizes between the ascending aorta and the autograft. Mean bypass and crossclamp times were 200.66 and 151.14 minutes, respectively. Median length of stay was 6 days. Mean follow-up was 16.88 months. Two patients required subsequent aortic valve replacement (1 had rheumatic valve disease and the other had iatrogenic damage in his autograft valve leaflet). Ascending aorta dimensions remain stable when compared with immediate postoperative studies. There were no deaths.
Conclusions: The ExoVasc PEARS graft has proven to be an excellent support in the Ross operation to prevent the autograft failure related to autograft dilatation that can offer several advantages compared with other existing techniques. With this type of support, we believe the Ross indications can be expanded to multiple clinical scenarios, given the good long-term results this operation offers in terms of durability, life expectancy, and hemodynamics.
Keywords: Personalized External Aortic Root Support; Ross; aortic root; aortic valve.
© 2024 The Author(s).
Conflict of interest statement
The authors reported no conflicts of interest. The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Figures




References
-
- Ross D. The Ross operation. J Card Surg. 2002;17:188–193. - PubMed
-
- El-Hamamsy I., Toyoda N., Itagaki S., et al. Propensity-matched comparison of the Ross procedure and prosthetic aortic valve replacement in adults. J Am Coll Cardiol. 2002;79:805–815. - PubMed
-
- Hraska V., Mitchell M.E., Woods R.K. Roadmap for Ross procedure: staged strategy. J Thorac Cardiovasc Surg. 2022;163(2):379–382. - PubMed
-
- Mazine A., El-Hamamsy I., Verma S., et al. Ross procedure in adults for cardiologists and cardiac surgeons: JACC State-of-the-Art Review. J Am Coll Cardiol. 2018;72(22):2761–2777. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
