

Effects of Low-Load Blood Flow Restriction Training on Rotator Cuff Strength and Hypertrophy: Case Series
- PMID: 38835981
- PMCID: PMC11144660
- DOI: 10.26603/001c.118143
Effects of Low-Load Blood Flow Restriction Training on Rotator Cuff Strength and Hypertrophy: Case Series
Abstract
Background: The rotator cuff (RC) plays a pivotal role in the performance and health of the shoulder and upper extremity. Blood flow restriction training (BFRT) is a modality to improve strength and muscle hypertrophy with even low-load training in healthy and injured individuals. There is minimal evidence examining its effect proximal to the occluded area, and particularly on the RC.
Hypothesis & purpose: The purpose of this case series is to explore the effects of low-load BFRT on RC strength, hypertrophy, and tendon thickness in asymptomatic individuals.
Study design: Case series.
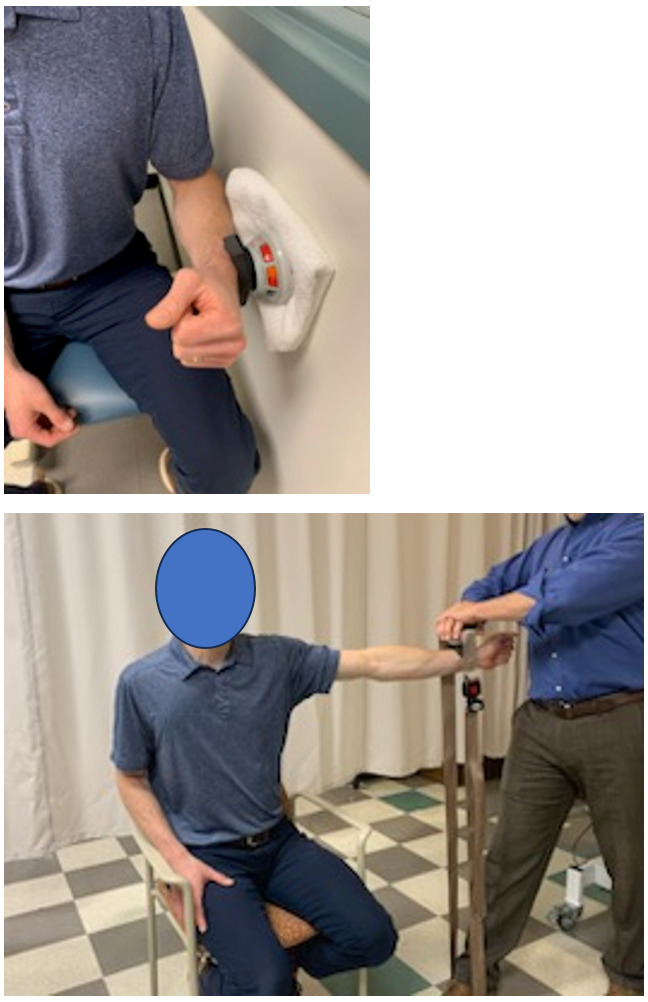
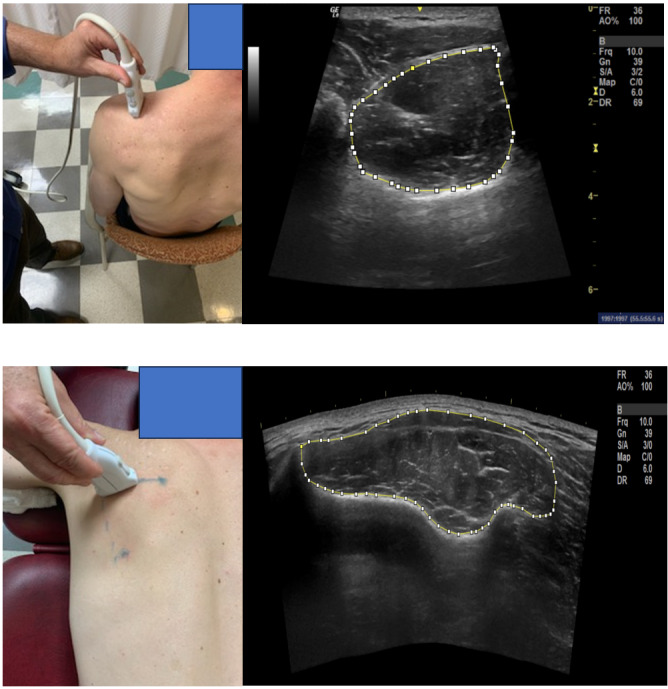
Methods: Fourteen participants with asymptomatic, untrained shoulders were recruited to participate. They performed an eight-week low-load shoulder exercise regimen where BFR was applied to the dominant arm only during exercise. The dependent variables were maximal isometric strength of the shoulder external rotators(ER) and elevators (in the scapular plane in full can position) (FC) measured via handheld dynamometry, cross sectional area (CSA) of the supraspinatus and infraspinatus muscles, and supraspinatus tendon thickness measured via ultrasound imaging (US). Mean changes within and between arms were compared after training using paired t-tests. Cohen's d was used to determine effect sizes.
Results: All participants were able to complete the BFRT regimen without adverse effects. Mean strength and CSA increased for all variables in both arms, however this increase was only significant (p\<0.01) for FC strength bilaterally and CSA for the supraspinatus and infraspinatus on the BFRT side. The effect sizes for increased supraspinatus and infraspinatus CSA on the BFRT side were 0.40 (9.8% increase) and 0.46 (11.7% increase) respectively. There were no significant differences when comparing the mean changes of the BFRT side to the non-BFRT side for strength or muscle CSA. There were no significant changes to supraspinatus tendon thickness.
Conclusion: These results suggest variability in response of the RC musculature to low-load BFRT in asymptomatic individuals. The potential for a confounding systemic response in the study design makes determining whether low-load BFRT is more beneficial than low-load non-BFRT difficult. The hypertrophy seen on the BFRT side warrants further study.
Level of evidence: 4.
Keywords: BFRT; blood flow restriction training; cross-sectional area; rotator cuff; shoulder.
© The Author(s).
Conflict of interest statement
All authors, their immediate family, and any research foundation with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials