

Venous Thromboembolic Events in Adult Trauma Patients Receiving Balanced Hemostatic Resuscitation (BHR): An Analysis of Their Incidence, Predictors, and Associated Mortality Rates at a Level 1 Trauma Center
- PMID: 38836163
- PMCID: PMC11149781
- DOI: 10.7759/cureus.59679
Venous Thromboembolic Events in Adult Trauma Patients Receiving Balanced Hemostatic Resuscitation (BHR): An Analysis of Their Incidence, Predictors, and Associated Mortality Rates at a Level 1 Trauma Center
Abstract
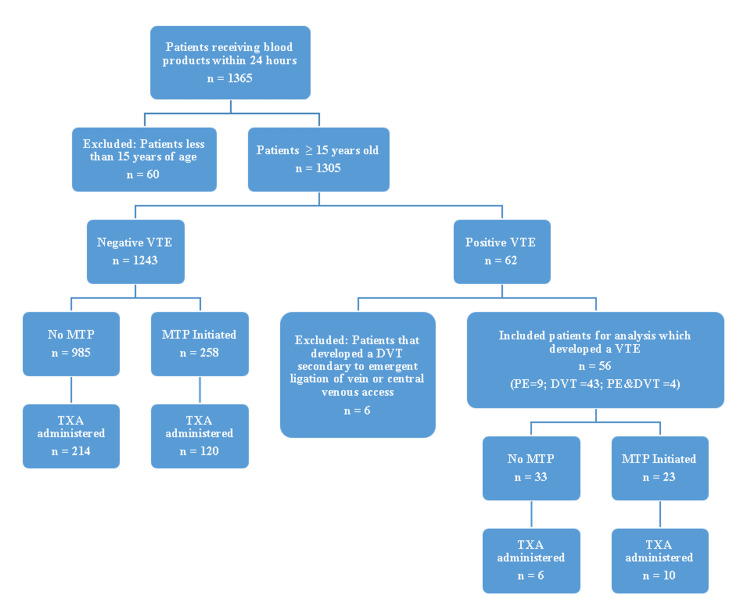
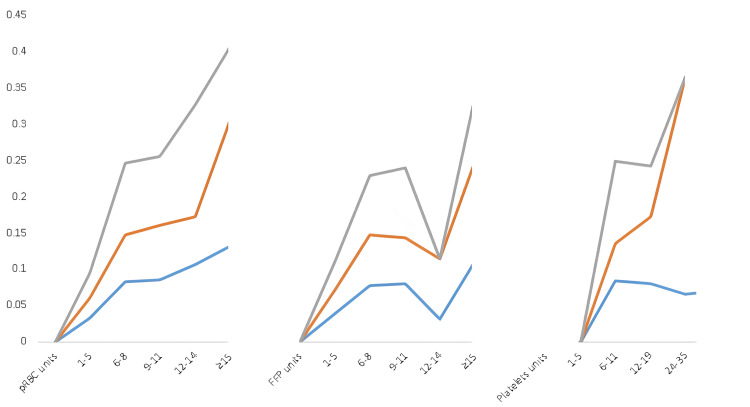
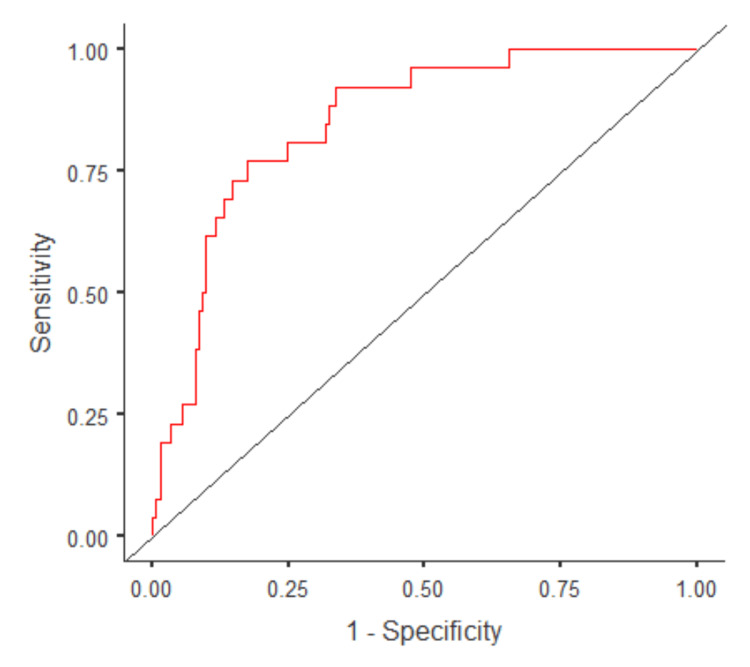
Background and objective Studies assessing the incidence of venous thromboembolic (VTE) events in the setting of massive balanced transfusions and/or tranexamic acid (TXA) infusion have yielded varied outcomes. In light of this, we conducted this study to examine the incidence of VTEs in trauma patients requiring blood products, and to identify the risk factors for VTE and mortality in this population. Methods We performed a retrospective analysis of trauma patients admitted to our level 1 trauma center from January 2013 to September 2023. Clinical characteristics were compared between patients who developed VTE and those who did not. A regression analysis of potential variables associated with the development of VTEs and mortality was performed. Results Among 1305 patients (mean age: 42.4 ± 18.8 years) receiving blood products within the initial 24 hours, 4.3% (56 patients) developed a VTE. Patients with VTE experienced prolonged ICU and hospital stays and ventilation duration (p<0.001). They were also noted to have delayed initiation of VTE prophylaxis (104.2 vs. 50.3 hours, p<.001). Prolonged ventilation >7 days was the sole significant factor associated with VTE in multivariate regression analysis [odds ratio (OR): 6.2, p=0.004]. Early TXA administration (within four hours) showed a higher association with VTE than TXA within 24 hours (OR: 2.1, p=0.07 vs. OR 1.6, p=0.22). Massive transfusion was found to increase VTE risk (OR: 2.65, p<0.001). Severe head and neck (OR: 6.0, p=0.002) and chest (OR: 3.8, p=0.01) injuries were key predictors of mortality, while TXA was not significantly associated with mortality in the multivariate model. Conclusions Our study revealed an elevated risk of VTE in patients requiring massive transfusion protocol (MTP, ≥6 units). Early TXA administration was neither associated with increased VTE risk in MTP patients nor increased mortality risk. Strategies directed at reducing the risk of VTE in massively transfused patients while maintaining the survival benefits of balanced resuscitation and TXA need to be devised.
Keywords: balanced resuscitation; massive transfusion; mortality; predictors; tranexamic acid; trauma; venous thromboembolism.
Copyright © 2024, Halalmeh et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Does tranexamic acid increase venous thromboembolism risk among trauma patients? A prospective multicenter analysis across 17 level I trauma centers.Injury. 2023 Nov;54(11):111008. doi: 10.1016/j.injury.2023.111008. Epub 2023 Aug 23. Injury. 2023. PMID: 37669883
-
Tranexamic acid administration is associated with an increased risk of posttraumatic venous thromboembolism.J Trauma Acute Care Surg. 2019 Jan;86(1):20-27. doi: 10.1097/TA.0000000000002061. J Trauma Acute Care Surg. 2019. PMID: 30239375
-
Prehospital administration of tranexamic acid in trauma patients: A 1:1 matched comparative study from a level 1 trauma center.Am J Emerg Med. 2020 Feb;38(2):266-271. doi: 10.1016/j.ajem.2019.04.051. Epub 2019 Apr 30. Am J Emerg Med. 2020. PMID: 31060862
-
Effect of tranexamic acid use on blood loss and thromboembolic risk in hip fracture surgery: systematic review and meta-analysis.Hip Int. 2018 Jan;28(1):3-10. doi: 10.5301/hipint.5000556. Hip Int. 2018. PMID: 28983887
-
A Systematic Review of Tranexamic Acid-Associated Venous Thromboembolic Events in Combat Casualties and Considerations for Prolonged Field Care.Mil Med. 2023 Aug 29;188(9-10):e2932-e2940. doi: 10.1093/milmed/usac317. Mil Med. 2023. PMID: 36315470
References
-
- Virchow's triad revisited. Brotman DJ, Deitcher SR, Lip GY, Matzdorff AC. South Med J. 2004;97:213–214. - PubMed
-
- Venous thromboembolism in trauma patients: a review. Rogers FB. Surgery. 2001;130:1–12. - PubMed
-
- Venous thromboembolism after severe trauma: incidence, risk factors and outcome. Paffrath T, Wafaisade A, Lefering R, et al. Injury. 2010;41:97–101. - PubMed
-
- Impact of hemorrhage on trauma outcome: an overview of epidemiology, clinical presentations, and therapeutic considerations. Kauvar DS, Lefering R, Wade CE. J Trauma. 2006;60:0–11. - PubMed
LinkOut - more resources
Full Text Sources