

Endovascular Therapy in the Extended Time Window for Large Vessel Occlusion in Patients With Pre-Stroke Disability
- PMID: 38836274
- PMCID: PMC11164586
- DOI: 10.5853/jos.2023.04259
Endovascular Therapy in the Extended Time Window for Large Vessel Occlusion in Patients With Pre-Stroke Disability
Abstract
Background and purpose: We compared the outcomes of endovascular therapy (EVT) in an extended time window in patients with large-vessel occlusion (LVO) between patients with and without pre-stroke disability.
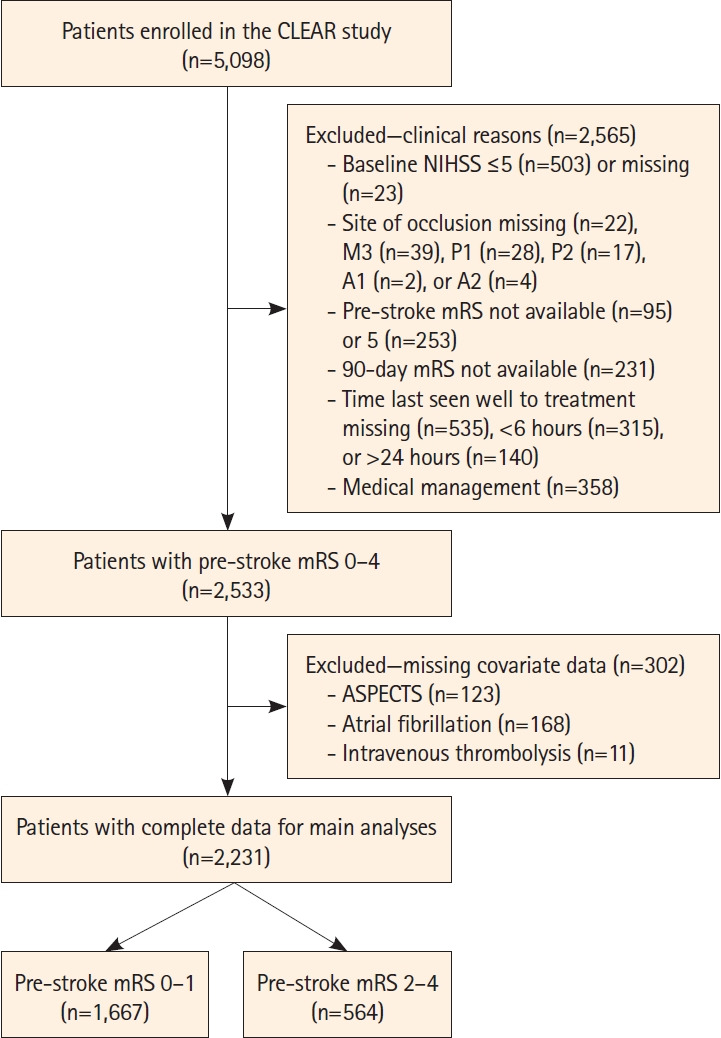
Methods: In this prespecified analysis of the multinational CT for Late Endovascular Reperfusion study (66 participating sites, 10 countries between 2014 and 2022), we analyzed data from patients with acute ischemic stroke with a pre-stroke modified Rankin Scale (mRS) score of 0-4 and LVO who underwent EVT 6-24 hours from the time last seen well. The primary outcome was the composite of functional independence (FI; mRS score 0-2) or return to the pre-stroke mRS score (return of Rankin, RoR) at 90 days. Outcomes were compared between patients with pre-stroke disability (pre-stroke mRS score 2-4) and those without (mRS score 0-1).
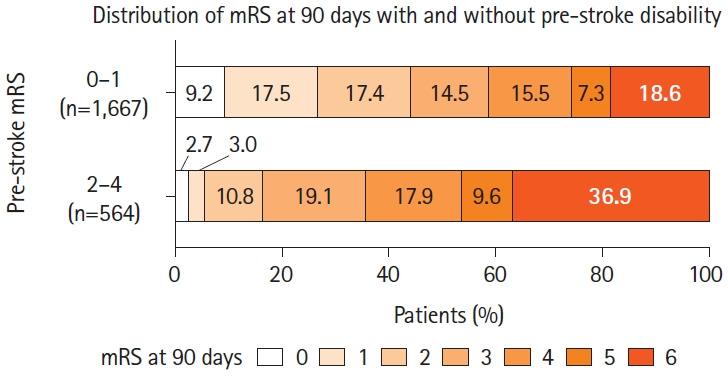
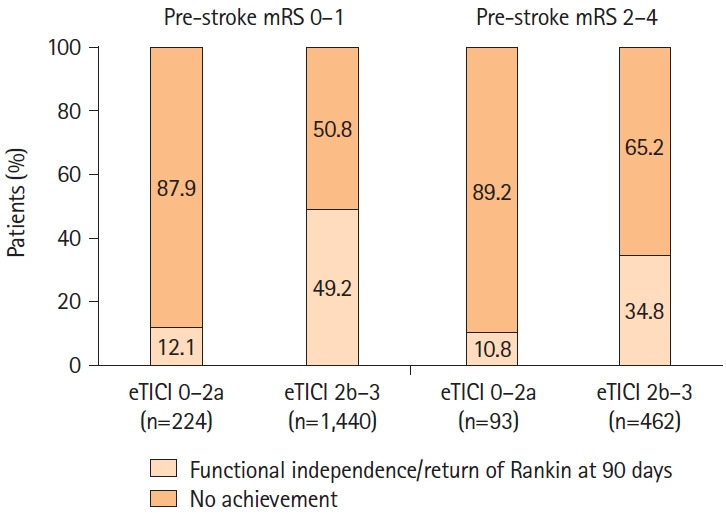
Results: A total of 2,231 patients (median age, 72 years; median National Institutes of Health Stroke Scale score, 16) were included in the present analysis. Of these, 564 (25%) had pre-stroke disability. The primary outcome (FI or RoR) was observed in 30.7% of patients with pre-stroke disability (FI, 16.5%; RoR, 30.7%) compared to 44.1% of patients without (FI, 44.1%; RoR, 13.0%) (P<0.001). In multivariable logistic regression analysis with inverse probability of treatment weighting, pre-stroke disability was not associated with significantly lower odds of achieving FI or RoR (adjusted odds ratio 0.73, 95% confidence interval 0.43-1.25). Symptomatic intracranial hemorrhage occurred in 6.3% of both groups (P=0.995).
Conclusion: A considerable proportion of patients with late-presenting LVO and pre-stroke disability regained pre-stroke mRS scores after EVT. EVT may be appropriate for patients with pre-stroke disability presenting in the extended time window.
Keywords: Activities of daily living; Endovascular therapy; Ischemic stroke; Outcome; Reperfusion.
Conflict of interest statement
H. Yamagami received research grants from Bristol-Myers Squibb; lecturer fees from Stryker, Medtronic, Johnson & Johnson, Bayer, Daiichi Sankyo, Bristol-Myers Squibb, and Otuska Pharmaceutical; and is an advisory board for Daiichi Sankyo. Siegler reported consultancy fees from Ceribell and involvement in the AstraZeneca Speakers Bureau. Nogueira reported consultancy fees from Biogen, Brainomix, Corindus, Cerenovus, Stryker, Medtronic, Ceretrieve, Anaconda, Biomed, Vesalio, Imperative Care, NeuroVasc Technologies, Viz AI, Genentech, Prolong Pharmaceuticals, Perfuze, Phenox, RapidPulse, and stock options in Viz AI, Vesalio, Perfuze, Corindus, Brainomix, and Ceretrieve, grants from Cerenovus and Stryker. S. Yoshimura reported research grants from Stryker, Siemens Healthineers, Bristol-Myers Squibb, Sanofi, Eisai, Daiichi Sankyo, Teijin Pharma, Chugai Pharmaceutical, HEALIOS, Asahi Kasei Medical, Kowa, CSL Behring and lecturer fees from Stryker, Medtronic, Johnson & Johnson, Kaneka, Terumo, Biomedical Solutions, Boehringer-Ingelheim, Daiichi Sankyo, Bayer and Bristol-Meyers Squibb. N. Sakai received a research grant from Biomedical Solutions, Medtronic, Terumo, and TG Medical; lecturer fees from Asahi-Intec, Biomedical Solutions, Daiichi-Sankyo, Kaneka, Medtronic, and Terumo; and is a member of the advisory boards for Johnson & Johnson, Medtronic, and Terumo. S. Nagel reported consultancy fees from Brainomix and is a speaker with Boehringer Ingelheim and Pfizer. V. Puetz reported lecturer fees from Daiichi Sankyo. Haussen reported consultancy fees from Vesalio, Cerenovus, Stryker, Brainomix, Poseydon Medical, and Chiesi, USA; DSMB from the Jacobs Institute; and stock options in Viz AI. J. P. Marto reported consultancy feed from Amicus Therapeutics and Boehringer Ingelheim and is a Speaker with Boehringer Ingelheim. Sheth reported consultancy fees from Imperative Care, Viz AI, Penumbra, compensation from Motif Neurosciences, and grants from the National Institutes of Health. J. Kaesmacher reported grants from the Swiss Academy of Medical Sciences/Bangerter Foundation, Swiss Stroke Society, and Clinical Trials Unit Bern. D. P. O. Kaiser reported grants from the Joachim Herz Foundation. M. A. Möhlenbruch reported grants from Medtronic, Stryker, and MicroVention. P. A. Ringleb reported travel support from Bayer and Bristol Myers Squibb, and a consultancy for Daiichi Sankyo Company, and Boehringer Ingelheim. M. Ribo reported consultancy fees from Medtronic, MiniMed, Cerenovus, AptaTargets, Stryker, Philips and stock holdings in Methinks, Nora, and Anaconda Biomed. P. Michel reported grants from the University of Lausanne and Swiss National Science Foundation (SNF). T. N. Nguyen disclosed research support from Medtronic to her institution; is a member of the advisory board for Idorsia, Brainomix; and is an Associate Editor of
Figures
Similar articles
-
Endovascular Therapy for Patients With Low NIHSS Scores and Large Vessel Occlusion in the 6- to 24-Hour Window: Analysis of the CLEAR Study.Neurology. 2025 Apr;104(7):e213442. doi: 10.1212/WNL.0000000000213442. Epub 2025 Mar 20. Neurology. 2025. PMID: 40112237
-
Endovascular vs Medical Management for Late Anterior Large Vessel Occlusion With Prestroke Disability: Analysis of CLEAR and RESCUE-Japan.Neurology. 2023 Feb 14;100(7):e751-e763. doi: 10.1212/WNL.0000000000201543. Epub 2022 Nov 4. Neurology. 2023. PMID: 36332983 Free PMC article.
-
Sex Differences in Outcomes of Late-Window Endovascular Stroke Therapy.Stroke. 2024 Feb;55(2):278-287. doi: 10.1161/STROKEAHA.123.045015. Epub 2024 Jan 22. Stroke. 2024. PMID: 38252759
-
Efficacy and safety of endovascular treatment with or without intravenous alteplase in acute anterior circulation large vessel occlusion stroke: a meta-analysis of randomized controlled trials.Neurol Sci. 2022 Jun;43(6):3551-3563. doi: 10.1007/s10072-022-06017-8. Epub 2022 Mar 22. Neurol Sci. 2022. PMID: 35314911 Review.
-
Endovascular treatment or general treatment: how should acute ischemic stroke patients choose to benefit from them the most?: A systematic review and meta-analysis.Medicine (Baltimore). 2020 May;99(20):e20187. doi: 10.1097/MD.0000000000020187. Medicine (Baltimore). 2020. PMID: 32443338 Free PMC article.
Cited by
-
CLEAR Thrombectomy Score: An Index to Estimate the Probability of Good Functional Outcome With or Without Endovascular Treatment in the Late Window for Anterior Circulation Occlusion.J Am Heart Assoc. 2024 Jul 16;13(14):e034948. doi: 10.1161/JAHA.124.034948. Epub 2024 Jul 9. J Am Heart Assoc. 2024. PMID: 38979812 Free PMC article.
-
Long-term outcome of endovascular thrombectomy in patients with acute ischemic stroke: a systematic review and meta-analysis.J Neurol. 2025 Jan 7;272(1):101. doi: 10.1007/s00415-024-12842-y. J Neurol. 2025. PMID: 39777553
-
Initial calf circumference predicts poor disability outcomes in patients with stroke.J Nutr Health Aging. 2025 Mar;29(3):100483. doi: 10.1016/j.jnha.2025.100483. Epub 2025 Jan 9. J Nutr Health Aging. 2025. PMID: 39793438 Free PMC article.
References
-
- Yamagami H, Hayakawa M, Inoue M, Iihara K, Ogasawara K, Toyoda K, et al. Guidelines for mechanical thrombectomy in Japan, the fourth edition, March 2020: a guideline from the Japan Stroke Society, the Japan Neurosurgical Society, and the Japanese Society for Neuroendovascular Therapy. Neurol Med Chir (Tokyo) 2021;61:163–192. - PMC - PubMed
-
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50:e344–e418. - PubMed
-
- Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al. Endovascular thrombectomy after largevessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387:1723–1731. - PubMed
-
- Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 2018;378:11–21. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
