

Enhanced Survival of 22-25 Week Preterm Infants After Proactive Care Implementation: A Comparative Analysis of Two Time Periods
- PMID: 38836963
- PMCID: PMC12279888
- DOI: 10.1007/s12098-024-05164-4
Enhanced Survival of 22-25 Week Preterm Infants After Proactive Care Implementation: A Comparative Analysis of Two Time Periods
Abstract
Objectives: To investigate the impact of proactive perinatal care on periviable preterm infants before and after its implementation.
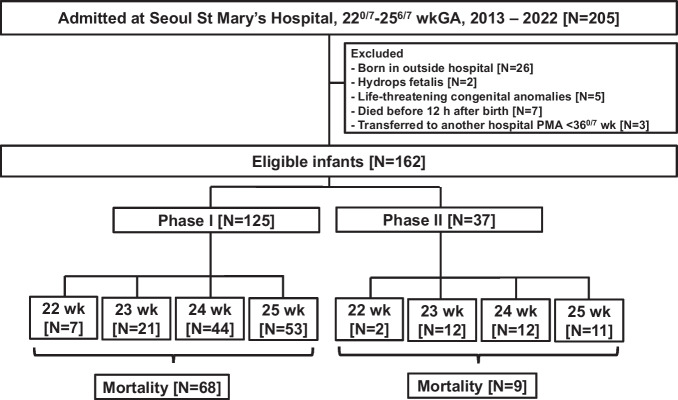
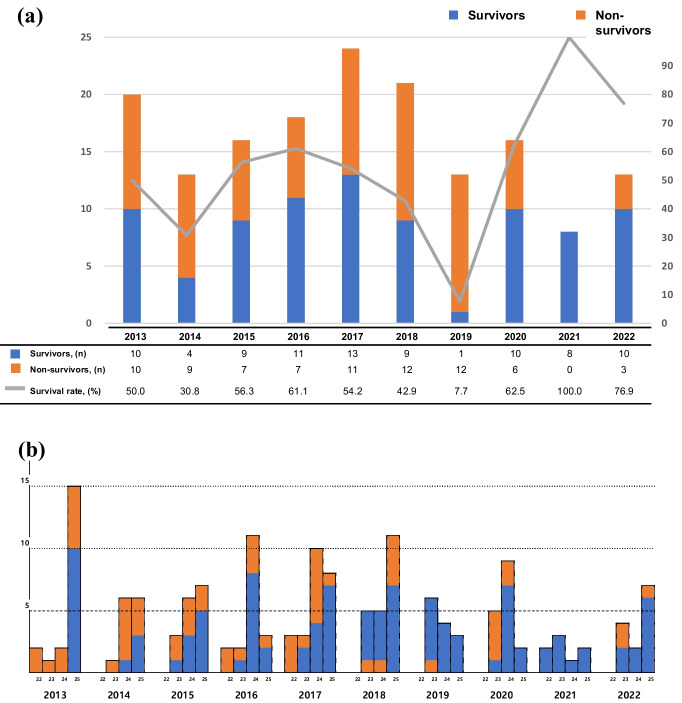
Methods: This retrospective cohort study was conducted over a period of 10 y, from 2013 to 2019, referred to as Phase I, and from 2020 to 2022, referred to as Phase II. A total of 162 eligible infants born between 220/7 and 256/7 wk of gestation were included in this analysis.
Results: A total of 125 infants were born in phase I, and 37 infants in phase II received proactive care with minimal handling. The mortality decreased from 54.4% to 24.3% (P = 0.001). The composite outcomes of severe brain injury or death, sepsis or death and necrotizing enterocolitis or death were also improved with proactive care. Gestational age [adjusted odds ratio (aOR) 0.900; 95% confidence interval (CI), 0.836-0.970], air leak syndrome (aOR 4.958; 95% CI, 1.681-14.624), massive pulmonary hemorrhage (aOR 4.944; 95% CI, 2.055-11.893), and birth in phase II (aOR 0.324; 95% CI, 0.115-0.912) were independently associated with mortality.
Conclusions: The implementation of proactive care with minimal handling resulted in an increased survival rate and a reduction in the combined morbidities between the two time periods. The provision of proactive perinatal care with minimal handling is crucial for improving both the survival rates and clinical outcomes of these vulnerable infants.
Keywords: Minimal handling; Mortality; Periviable preterm infant; Proactive perinatal care.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethical Approval: This study was approved by the Institutional Review Board (IRB) of Seoul St. Mary's Hospital (IRB No. KC21TISI0329). Informed consent from the parents of study participants was waived because of retrospective design with minimal risk. Conflict of Interest: None.
Figures
References
-
- American College of Obstetricians and Gynecologists and the Society for Maternal–Fetal Medicine; Ecker JL, Kaimal A, Mercer BM, et al. # 3: Periviable birth. Am J Obstet Gynecol. 2015;213:604–14. - PubMed
-
- Raju TNK, Mercer BM, Burchfield DJ, Joseph GF Jr. Periviable birth: executive summary of a joint workshop by the Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, American Academy of Pediatrics, and American College of Obstetricians and Gynecologists. Am J Obstet Gynecol. 2014;210:406–17. - PubMed
-
- Lantos JD, Meadow W. Variation in the treatment of infants born at the borderline of viability. Pediatrics. 2009;123:1588–90. - PubMed
-
- García-Muñoz Rodrigo F, Diez Recinos AL, Garcia-Alix Perez A, Figueras Aloy J, Vento Torres M. Changes in perinatal care and outcomes in newborns at the limit of viability in Spain: the EPI-SEN Study. Neonatology. 2015;107:120–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
