

Successful R0 resection after chemotherapy, including nivolumab, for gastric cancer with liver metastases: three case reports
- PMID: 38837046
- PMCID: PMC11153382
- DOI: 10.1186/s40792-024-01929-3
Successful R0 resection after chemotherapy, including nivolumab, for gastric cancer with liver metastases: three case reports
Abstract
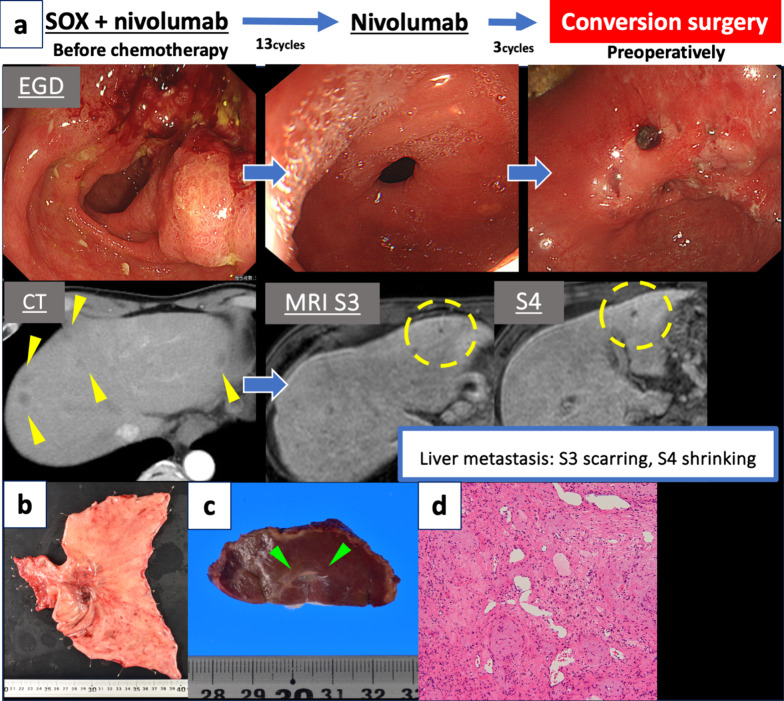
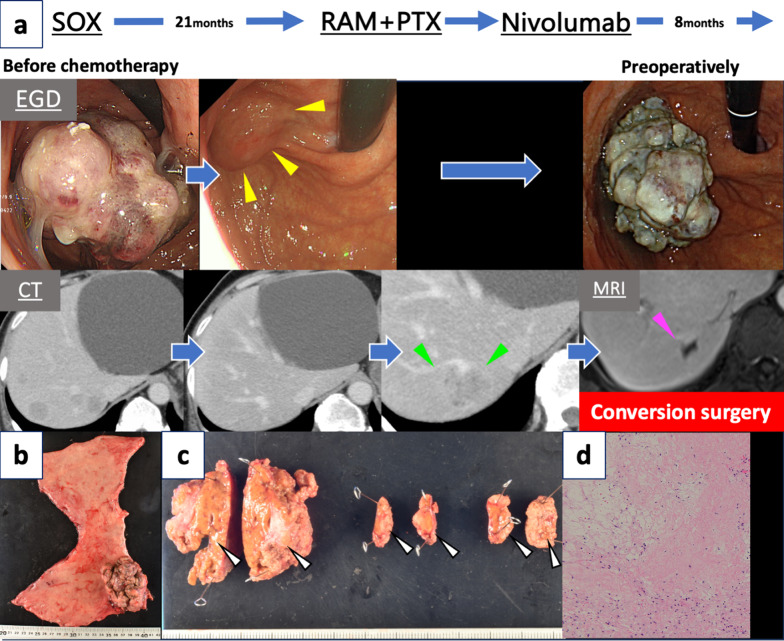
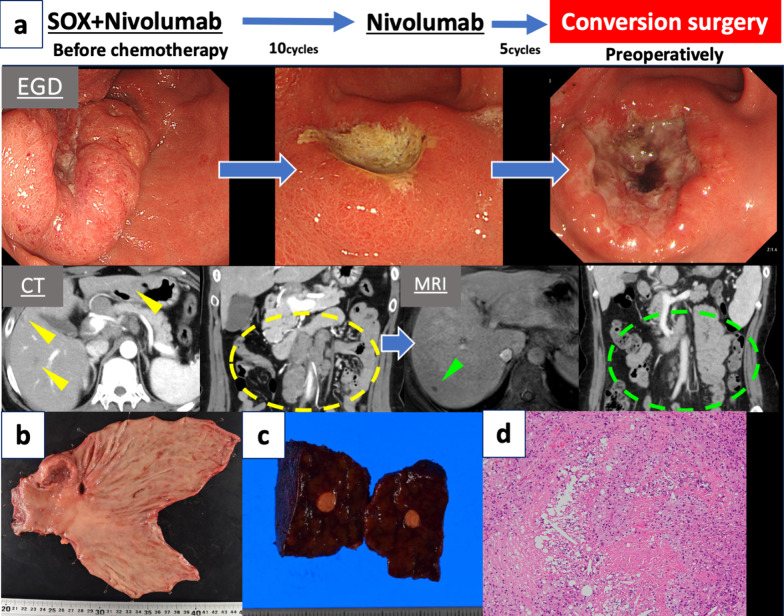
Background: Advances in chemotherapy have increased clinical experience with conversion surgery for inoperable advanced gastric cancer. This report describes three patients with unresectable gastric cancer accompanied by multiple liver metastases. In all three patients, nivolumab resolved the liver metastases and subsequent conversion surgery achieved a pathological complete response.
Case presentation: In Case 1, a 68-year-old man with clinical Stage IVB gastric cancer and multiple liver metastases initiated first-line therapy with SOX plus nivolumab. The patient completed 13 cycles; however, only nivolumab was continued for 3 cycles because of adverse events. Distal gastrectomy and partial hepatic resection were performed because of a significant reduction in the size of the liver metastases as observed on magnetic resonance imaging (MRI). In Case 2, a 72-year-old man with clinical Stage IVB gastric cancer and multiple liver metastases initiated first-line therapy with SOX. Because of the subsequent emergence of new liver metastases, the patient transitioned to ramucirumab plus paclitaxel as second-line therapy. Third-line therapy with nivolumab was initiated because of side effects. MRI revealed necrosis within the liver metastasis, and the patient underwent proximal gastrectomy and partial hepatectomy. In Case 3, a 51-year-old woman with clinical Stage IVB gastric cancer accompanied by multiple metastases of the liver and para-aortic lymph nodes began first-line therapy with SOX plus nivolumab. The patient completed 10 cycles; however, only nivolumab was continued for 5 cycles because of adverse events. Computed tomography showed a significant decrease in the size of the para-aortic lymph nodes, while MRI indicated the presence of a singular liver metastasis. Distal gastrectomy and partial hepatic resection were subsequently performed. In all three cases, MRI revealed the presence of liver metastases; however, pathological examination showed no viable tumor cells.
Conclusions: We herein present three cases in which chemotherapy, including nivolumab, elicited a response in patients with multiple unresectable liver metastases, ultimately culminating in R0 resection through conversion surgery. Although MRI showed liver metastases, pathological analysis revealed no cancer, underscoring the beneficial impact of chemotherapy.
Keywords: Complete response; Conversion surgery; Gastric cancer; Liver metastases; Nivolumab.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Conversion surgery for stage IV gastric cancer with a complete pathological response to nivolumab: a case report.World J Surg Oncol. 2020 Jul 21;18(1):179. doi: 10.1186/s12957-020-01954-0. World J Surg Oncol. 2020. PMID: 32693806 Free PMC article.
-
Conversion surgery for gastric remnant cancer with liver metastasis after nivolumab combination chemotherapy achieving pathological complete response: a case report and literature review.Surg Case Rep. 2024 May 1;10(1):107. doi: 10.1186/s40792-024-01905-x. Surg Case Rep. 2024. PMID: 38691201 Free PMC article.
-
Successful management of multiple liver metastasis from gastric cancer with second conversion surgery: A case report.Int J Surg Case Rep. 2023 Jun;107:108340. doi: 10.1016/j.ijscr.2023.108340. Epub 2023 May 19. Int J Surg Case Rep. 2023. PMID: 37216732 Free PMC article.
-
[Clinical significance and efficacy of conversion surgery for patients with stage IV gastric cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2018 Oct 25;21(10):1087-1092. Zhonghua Wei Chang Wai Ke Za Zhi. 2018. PMID: 30370504 Review. Chinese.
-
[A Case of Neuroendocrine Carcinoma of the Stomach Treated with TAS-102].Gan To Kagaku Ryoho. 2022 Oct;49(10):1109-1111. Gan To Kagaku Ryoho. 2022. PMID: 36281604 Review. Japanese.
Cited by
-
Identifying beneficial gastric cancer patient on prognosis after treating with perioperative or postoperative-only chemotherapy: a single-center real-world study.World J Surg Oncol. 2025 May 4;23(1):177. doi: 10.1186/s12957-025-03827-w. World J Surg Oncol. 2025. PMID: 40320534 Free PMC article.
-
Conversion hepatectomy after chemotherapy including nivolumab for multiple liver metastases of hepatoid adenocarcinoma of the stomach: A case report and literature review.Int J Surg Case Rep. 2024 Dec;125:110591. doi: 10.1016/j.ijscr.2024.110591. Epub 2024 Nov 15. Int J Surg Case Rep. 2024. PMID: 39571234 Free PMC article.
References
-
- Janjigian YY, Shitara K, Moehler M, Garrido M, Salman P, Shen L, et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. Lancet. 2021;398:27–40. doi: 10.1016/S0140-6736(21)00797-2. - DOI - PMC - PubMed
-
- Kang YK, Chen LT, Ryu MH, Oh DY, Oh SC, Chung HC, et al. Nivolumab plus chemotherapy versus placebo plus chemotherapy in patients with HER2-negative, untreated, unresectable advanced or recurrent gastric or gastro-oesophageal junction cancer (ATTRACTION-4): a randomised, multicentre, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2022;23:234–247. doi: 10.1016/S1470-2045(21)00692-6. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
