

Pulmonary hypertension across the spectrum of left heart and lung disease
- PMID: 38837273
- PMCID: PMC11269034
- DOI: 10.1002/ejhf.3302
Pulmonary hypertension across the spectrum of left heart and lung disease
Abstract
Aims: Patients with pulmonary hypertension (PH) are grouped based upon clinical and haemodynamic characteristics. Groups 2 (G2, left heart disease [LHD]) and 3 (G3, lung disease or hypoxaemia) are most common. Many patients display overlapping characteristics of heart and lung disease (G2-3), but this group is not well-characterized.
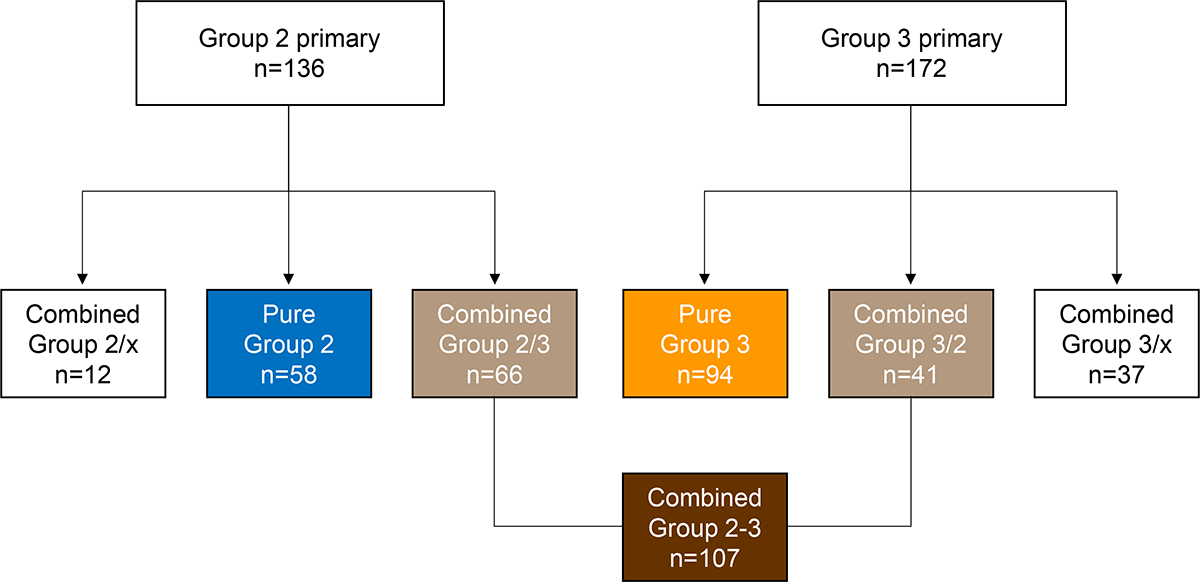
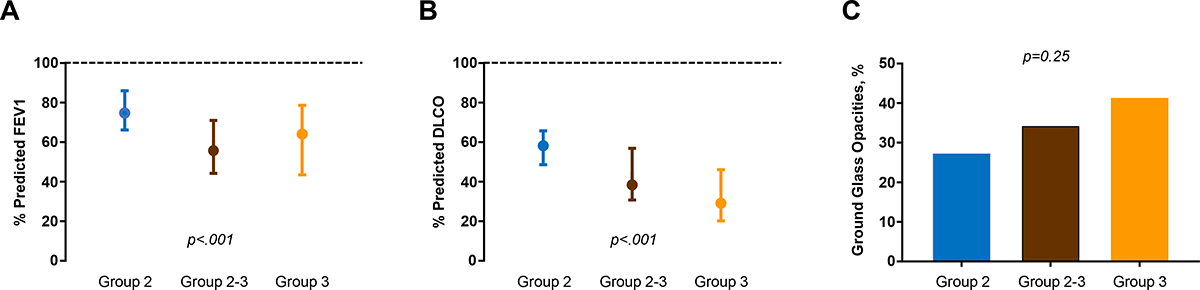
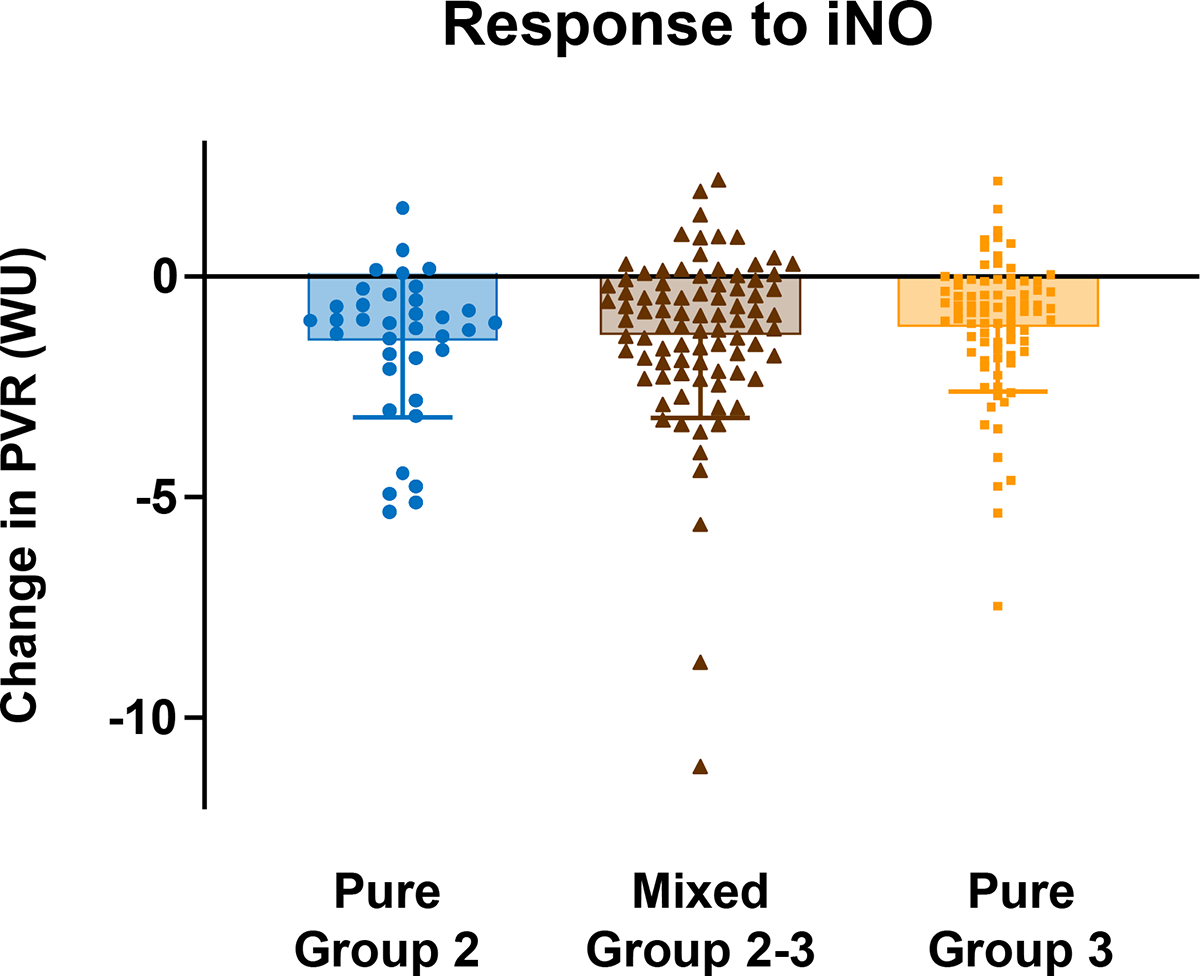
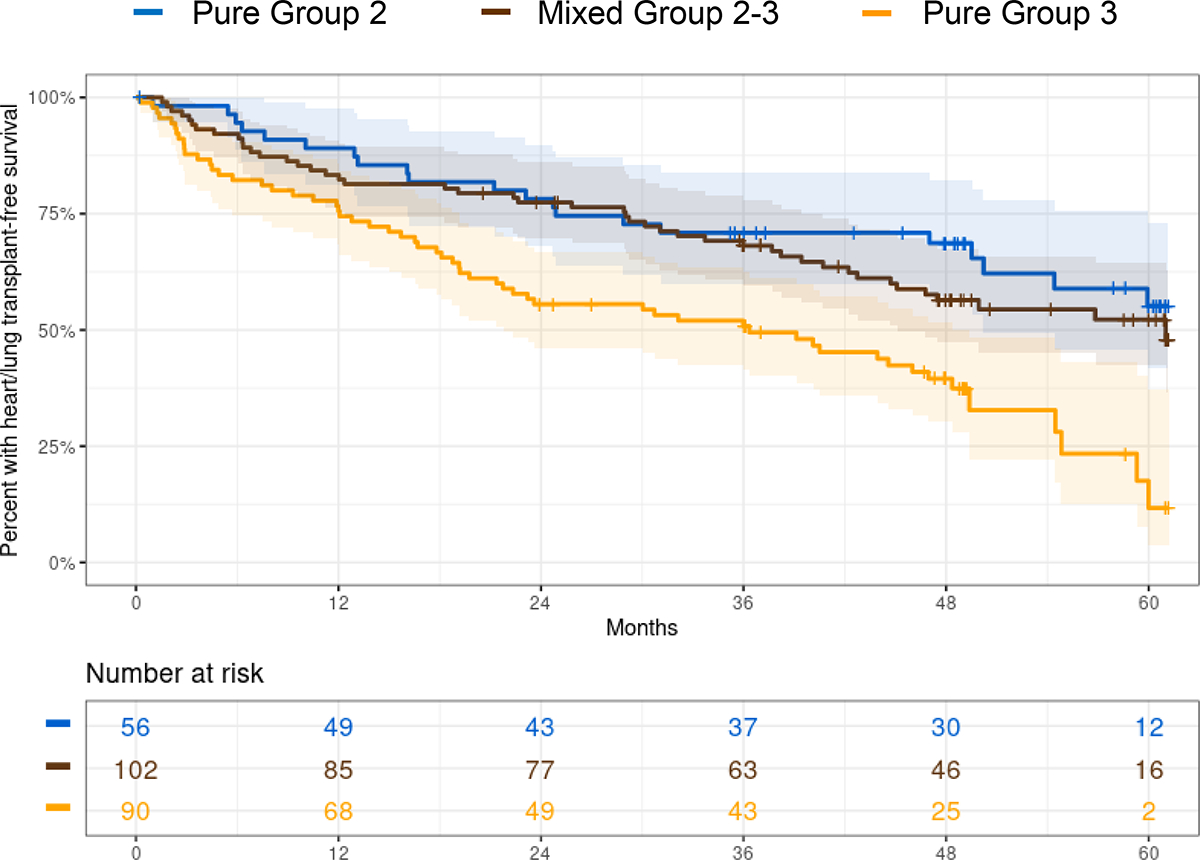
Methods and results: Patients with PH enrolled in the prospective, NHLBI-sponsored PVDOMICS network underwent intensive clinical, biomarker, imaging, gas exchange and exercise phenotyping. Patients with pure G2, pure G3, or overlapping G2-3 PH were compared across multiple phenotypic domains. Of all patients with predominant G2 (n = 136), 66 (49%) were deemed to have secondary lung disease/hypoxaemia contributors (G2/3), and of all patients categorized as predominant G3 (n = 172), 41 (24%) were judged to have a component of secondary LHD (G3/2), such that 107 had G2-3 (combined G2/3 and G3/2). As compared with G3, patients with G2 and G2-3 were more obese and had greater prevalence of hypertension, atrial fibrillation, and coronary disease. Patients with G2 and G2-3 were more anaemic, with poorer kidney function, more cardiac dysfunction, and higher N-terminal pro-B-type natriuretic peptide than G3. Lung diffusion was more impaired in G3 and G2-3, but commonly abnormal even in G2. Exercise capacity was severely and similarly impaired across all groups, with no differences in 6-min walk distance or peak oxygen consumption, and pulmonary vasoreactivity to nitric oxide did not differ. In a multivariable Cox regression model, patients with G2 had lower risk of death or transplant compared with G3 (hazard ratio [HR] 0.51, 95% confidence interval [CI] 0.30-0.86), and patients with G2-3 also displayed lower risk compared with G3 (HR 0.57, 95% CI 0.38-0.86).
Conclusions: Overlap is common in patients with a pulmonary or cardiac basis for PH. While lung structure/function is clearly more impaired in G3 and G2-3 than G2, pulmonary abnormalities are common in G2, even when clinically judged as isolated LHD. Further study is required to identify optimal systematic evaluations to guide therapeutic innovation for PH associated with combined heart and lung disease.
Clinical trial registration: ClinicalTrials.gov NCT02980887.
Keywords: Combined post‐ and pre‐capillary pulmonary hypertension; Heart failure; Left heart disease; Lung disease; Pulmonary hypertension; Pulmonary vascular resistance.
© 2024 European Society of Cardiology.
Figures
Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Impact of residual disease as a prognostic factor for survival in women with advanced epithelial ovarian cancer after primary surgery.Cochrane Database Syst Rev. 2022 Sep 26;9(9):CD015048. doi: 10.1002/14651858.CD015048.pub2. Cochrane Database Syst Rev. 2022. PMID: 36161421 Free PMC article.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
-
Phenotyping exercise limitation of patients with Interstitial Fibrosing Lung Disease: the importance of exercise hemodynamics.Pulmonology. 2024 Mar-Apr;30(2):104-112. doi: 10.1016/j.pulmoe.2022.03.012. Epub 2022 May 11. Pulmonology. 2024. PMID: 35568651
Cited by
-
Physiologic Phenotyping of Responses to Exercise and Activity in Heart Failure.Circ Res. 2025 Jul 7;137(2):290-315. doi: 10.1161/CIRCRESAHA.125.325534. Epub 2025 Jul 3. Circ Res. 2025. PMID: 40608855 Review.
-
Pulmonary hypertension aetiologies in different parts of the world.Int J Cardiol Congenit Heart Dis. 2025 Apr 15;20:100586. doi: 10.1016/j.ijcchd.2025.100586. eCollection 2025 Jun. Int J Cardiol Congenit Heart Dis. 2025. PMID: 40330318 Free PMC article. Review.
-
Defining Echocardiographic Degrees of Right Heart Size and Function in Pulmonary Vascular Disease from the PVDOMICS Study.Circ Cardiovasc Imaging. 2024 Oct;17(10):e017074. doi: 10.1161/circimaging.124.017074. Epub 2024 Oct 15. Circ Cardiovasc Imaging. 2024. PMID: 39691460
-
Hemodynamic Definitions, Phenotypes, Pathophysiology, and Evaluation of Pulmonary Hypertension Related to Left Heart Disease.J Cardiovasc Dev Dis. 2025 Jun 22;12(7):238. doi: 10.3390/jcdd12070238. J Cardiovasc Dev Dis. 2025. PMID: 40710764 Free PMC article. Review.
References
-
- Wijeratne DT, Lajkosz K, Brogly SB, Lougheed MD, Jiang L, Housin A, Barber D, Johnson A, Doliszny KM, Archer SL. Increasing Incidence and Prevalence of World Health Organization Groups 1 to 4 Pulmonary Hypertension: A Population-Based Cohort Study in Ontario, Canada. Circ Cardiovasc Qual Outcomes. 2018;11:e003973. doi: 10.1161/CIRCOUTCOMES.117.003973 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U01 HL125215/GF/NIH HHS/United States
- U01 HL125218/HL/NHLBI NIH HHS/United States
- U01 HL125175/HL/NHLBI NIH HHS/United States
- U01 HL125175/GF/NIH HHS/United States
- U01 HL125218/GF/NIH HHS/United States
- U01 HL125208/GF/NIH HHS/United States
- U01 HL125212/GF/NIH HHS/United States
- U01 HL125205/HL/NHLBI NIH HHS/United States
- U01 HL125177/HL/NHLBI NIH HHS/United States
- U01 HL125215/HL/NHLBI NIH HHS/United States
- U01 HL125208/HL/NHLBI NIH HHS/United States
- U01 HL125177/GF/NIH HHS/United States
- U01 HL125205/GF/NIH HHS/United States
- Pulmonary Hypertension Association
- U01 HL125212/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
